Dr. John Campbell is an internet sensation, giving facts & data to help us navigate healthcare in the present day. The interview covers John’s development, work, rise to fame & what he would do to help get healthcare back in shape.
Testing
A lot has been made about testing for COVID-19 but it is far from straightforward. There are many publicly acknowledged problems with testing procedures and accuracy of the results. Statistician Nate Silver writes, numbers are meaningless unless you understand how they’re counted.
Browse the articles related to this topic below.
Join our community on Guilded.
Speaking this week on The Mail on Sunday’s Medical Minefield podcast, Prof Woolhouse said: ‘I think that lockdown will be viewed by history as a monumental mistake on a global scale, for a number of reasons.
‘The obvious one is the immense harm the lockdown, more than any other measure, did in terms of the economy, mental health and on the wellbeing of society.
…[A study published in Science in February 2021] also found something intriguing: lockdowns could, in a worst-case scenario, actually increase transmission of the virus by up to five per cent.
…As Dr Ali puts it: ‘Some people say lockdowns were beneficial, others that they were really terrible.‘The reality actually is much closer to the idea that it didn’t make much difference either way.’
For those who made painful sacrifices, that won’t be an easy truth to swallow.
It has been one of the most enduring Covid conspiracy theories: that the ‘gold standard’ PCR tests used to diagnose the virus were picking up people who weren’t actually infected.
Some even suggested the swabs, which have been carried out more than 200 million times in the UK alone, may mistake common colds and flu for corona.
If either, or both, were true, it would mean many of these cases should never have been counted in the daily tally – that the ominous and all-too-familiar figure, which was used to inform decisions on lockdowns and other pandemic measures, was an over-count.
And many of those who were ‘pinged’ and forced to isolate as a contact of someone who tested positive – causing a huge strain on the economy – did so unnecessarily.
Such statements, it must be said, have been roundly dismissed by top experts. And those scientists willing to give credence such concerns have been shouted down on social media, accused of being ‘Covid-deniers’, and even sidelined by colleagues.
But could they have been right all along?
A senior epidemiologist who advised the government during the coronavirus pandemic claims he was told to “correct” his views after he criticised what he thought was an “implausible” graph shown at an official briefing.
Professor Mark Woolhouse has also apologised to his daughter, whose generation “has been so badly served by mine”, and believes that closing schools was “morally wrong”.
The Edinburgh University academic is deeply critical of the use of lockdown measures and says “plain common sense” was a “casualty of the crisis”.
Speaking to Sky News, Prof Woolhouse seemed concerned about a possible “big-brother” approach to the control of information about COVID.He says he was told to watch what he was saying following a briefing given by Chief Scientific Adviser (CSA) Sir Patrick Vallance on 21 September 2020.
Peter McCullough, MD, MPH speaks at the 78th Annual Meeting of AAPS on October 2, 2021.
Presentation notes:
- 1min: Something was going very wrong very early in 2019.
- 2m: The threshold for shutting down a new biologic product is just a few cases.
- 3m: Covid-19 was going to be the showcase of what we could do for biotech.
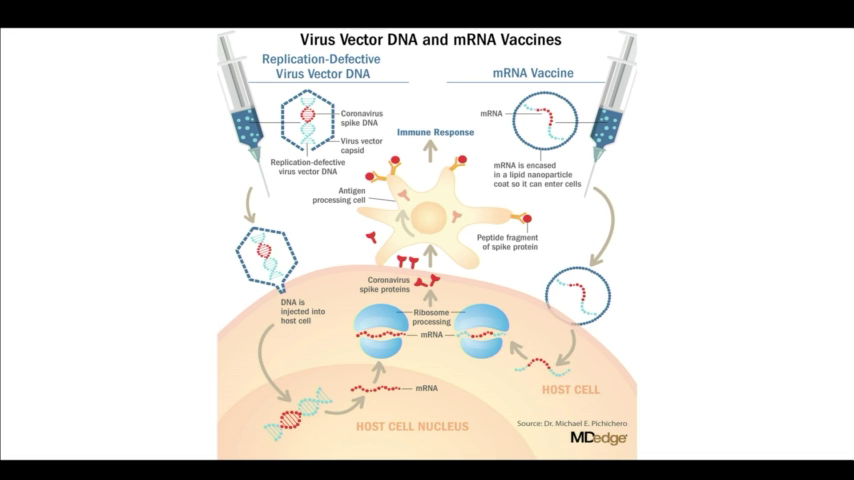
- 5m: The spike protein created by the new Covid-19 is a deadly protein.
- 11m: Our institutions are all culpable in medical malfeasance.
- 13m: We have the biggest biological catastrophe on our hands with a medicinal product in human history…and no-one knows how to stop it.
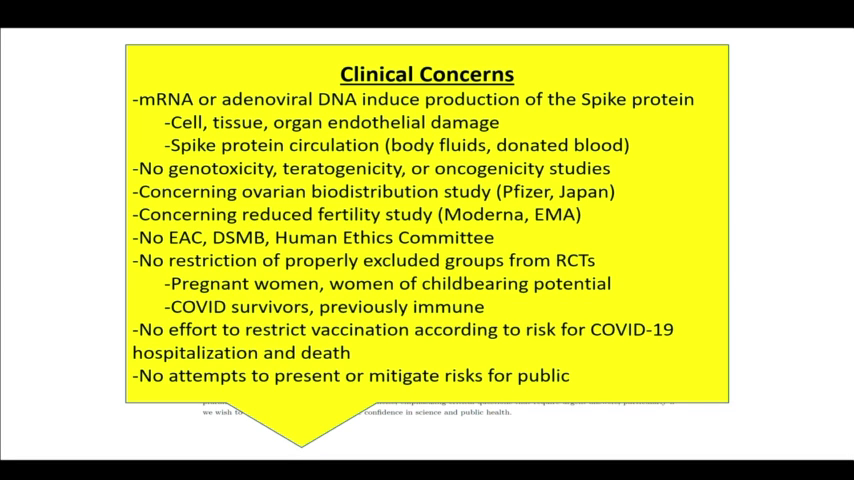
- List of risk
- 14m: 86% of deaths have no other explanation other than the vaccines.
- 20m: We are in freefall into a lawless state. The Vaccines are not safe for use on either side of the Atlantic. It’s clear that this first generation of [Covid-19] vaccines is not safe.
- 22m: The FDA did not approve Pfizer. The gave a continuation of the emergency use authorization and then conditionally approved Comirnaty with BioNTech which is legally and potentially medicinally distinct. The Pfizer approval is a false talking point.
- 23m: When Pfizer came up for boosters, McCullough and his team presented at the FDA showing that death with the vaccine is greater than death just taking your chances with the infection. The vaccines aren’t safe across the board and the panel agreed 16:2 against the booster.
- 26m: Data for the efficacy of the vaccines do not take into account the Delta variant. These vaccines have failed against Delta and other variants. Two-thirds who get sick with Delta are fully vaccinated. Data shows that the vaccines can’t stop transmission.
- 27m: Effectiveness for Pfizer is at 42%. A vaccine that falls below 50% protection and can’t last a year is not a viable product. Pfizer has failed as a commercial product.
- 29m: The CDC was telling us in May 2021 that the vaccines were failing. They started to do asymmetric reporting to craft a narrative that this was going to be a crisis of the unvaccinated but the CDC data showed the opposite. The ineptitude and willful misconduct of the people running our public health agencies is astounding.
- 32m: The ‘99% of hospitalized were unvaccinated’ message was a propagandized false talking point because the data is not there.
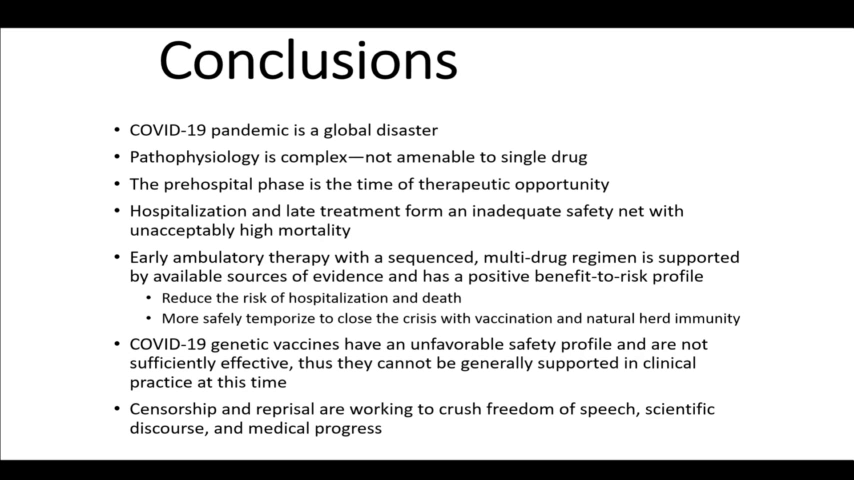
- 33m: The vaccines have had zero impact on the epidemic curve. Mortality is a function of treatment.
- 34m: Many experts have been warning that we shouldn’t vaccinate into a pandemic because it creates resistance. As soon as we started vaccinating, the number of strains starting falling. The virus was figuring out how to thrive in the vaccinated.
- 36m: The Delta variant has achieved antigenic escape. The data shows that the vaccinated is an equal threat to the unvaccinated.
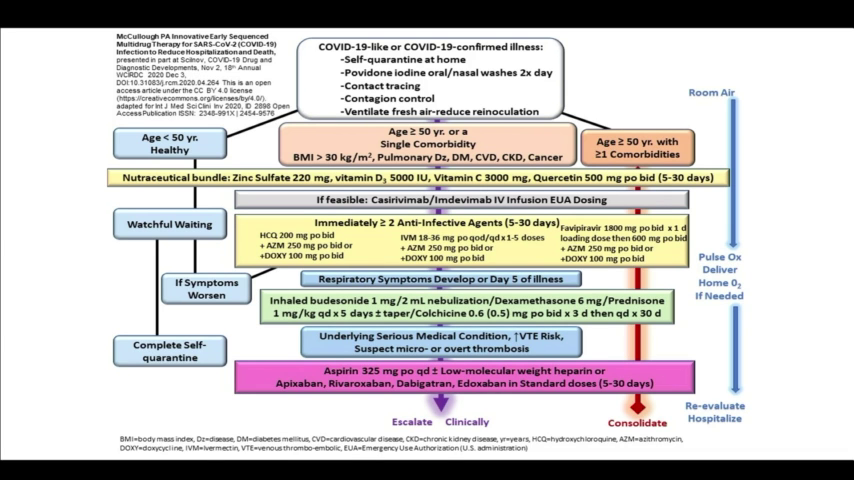
- 38m: Early home treatment is the only thing that makes sense. That’s what it should have always been.
- 40m: Doctors at my institution cannot look me in the eye because they are so ashamed of what they’ve done during the course of this pandemic.
- 44m: If you look through the clinical records [of those who have died] and I will tell you they were all inadequately treated.
- 50m: Natural immunity is superior to vaccine immunity. If we vaccinate people who are covid-recovered, we harm them considerably. The only backstop is natural immunity.
File download:
A Guide to Home-Based COVID Treatment from the Association of American Physicians and Surgeons – PDF (1.4MiB)
Slides:
Backup mirrors:
Dr. Hodkinson, here to discuss the dangers of the COVID-19 vaccines, the possibility of infertility, and the very real concerns about the vaccine-induced spike proteins and what new scientific research is clearly suggesting about their risks to your health.
Rob Verkerk, Founder, Executive and Scientific Director of the Alliance for Natural Health International, a scientist who has for 30 years been exploring positive ways to span the gulfs between science and the law, between academia and industry, and between governments and their people.
Backup mirror:
Undercover filming, by BBC Panorama, at a major UK Covid testing lab has revealed how poor working practices could lead to people getting incorrect test results.
Most people infected with SARS-CoV-2 are contagious for 4–8 days.7 Specimens are generally not found to contain culture-positive (potentially contagious) virus beyond day 9 after the onset of symptoms, with most transmission occurring before day 5. This timing fits with the observed patterns of virus transmission (usually 2 days before to 5 days after symptom onset), which led public health agencies to recommend a 10-day isolation period. The short window of transmissibility contrasts with a median 22–33 days of PCR positivity (longer with severe infections and somewhat shorter among asymptomatic individuals). This suggests that 50–75% of the time an individual is PCR positive, they are likely to be post-infectious.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00425-6/fulltext
Let’s dig deeper into PCR tests once again and have a look behind the curtain of this Covid-19 pandemic.
Ivor Cummins aka the Fat Emperor – gives James the lowdown on why you can’t trust anything our governments tell us about Covid-19. If you want the facts on Coronavirus – how deadly is it? do lockdowns and masks work? how does it compare with previous pandemics? – you’ve come to the right place
Please support the Delingpod:
Mirror archives are available below if this video is removed from YouTube.
I believe I have identified a serious, really a fatal flaw in the PCR test used in what is called by the UK Government the Pillar 2 screening – that is, testing many people out in their communities. I’m going to go through this with care and in detail because I’m a scientist and dislike where this investigation takes me.
…In the last 40 years alone the UK has had seven official epidemics/pandemics; AIDS, Swine flu, CJD, SARS, MERS, Bird flu as well as annual, seasonal flu. All were very worrying but schools remained open and the NHS treated everybody and most of the population were unaffected. The country would rarely have been open if it had been shut down every time.
Rising cases of the common cold could be giving a false picture of the spread of coronavirus among children.
Public Health England’s weekly coronavirus report shows a rise of almost 23% in rhinovirus infections, which include the common cold, in the last week.
But where did this one percent figure come from? You may find this hard to believe, but this figure emerged by mistake. A pretty major thing to make a mistake about, but that’s what happened.
In order to understand what happened, you have to understand the difference between two medical terms that sound the same – but are completely different. [IFR and CFR.]
CFR will always be far higher than the IFR. With influenza, the CFR is around ten times as high as the IFR. Covid seems to have a similar proportion.
Now, clearly, you do not want to get these figures mixed up. By doing so you would either wildly overestimate, or wildly underestimate, the impact of Covid. But mix these figures up, they did.
…we’ve had all the deaths we were ever going to get. And which also means that lockdown achieved, almost precisely nothing with regard to Covid. No deaths were prevented.
The main test used to diagnose coronavirus is so sensitive it could be picking up fragments of dead virus from old infections, scientists say.
Most people are infectious only for about a week, but could test positive weeks afterwards.
Researchers say this could be leading to an over-estimate of the current scale of the pandemic.
But some experts say it is uncertain how a reliable test can be produced that doesn’t risk missing cases.
Prof Carl Heneghan, one of the study’s authors, said instead of giving a “yes/no” result based on whether any virus is detected, tests should have a cut-off point so that very small amounts of virus do not trigger a positive result.
He believes the detection of traces of old virus could partly explain why the number of cases is rising while hospital admissions remain stable.
Nine out a 10 people in England live in areas that have not seen a Covid-19 case in a month and new lockdowns are not needed, an expert has said.
Professor John Clancy, from Birmingham University, has warned that fears of another shutdown are based on ‘dodgy data.’
Writing in a blog, he said: ”91 per cent of England (that’s 51million people) live in neighbourhoods where there hasn’t been a recorded Covid-19 case in the last 4 weeks.’
He added: ‘So-called ‘spikes’ are occurring here, there, and everywhere up and down the country because new testing regimes are causing them either with false positives, picking up residual infections or (usually more likely) suddenly increased testing in specific areas.’
CORONAVIRUS hospital admissions were over-counted at the peak of the pandemic as recovered patients returning to wards without Covid were included in the stats.
An investigation for the Government’s Science Advisory Group for Emergencies (Sage) found that people were being counted as ‘Covid hospital admissions’ if they had EVER had the virus.
Government figures show that, at the peak of the pandemic in early April, nearly 20,000 people a week were being admitted to hospital with coronavirus – but the true figure is now unknown because of the problem with over-counting.
This over-counting mirrors the problems with data for coronavirus deaths – where people who had died of other causes were being included in Covid-19 statistics if they had once tested positive.
Professor Graham Medley, of the London School of Hygiene and Tropical Medicine, asked by Sage to look into the situation, told The Telegraph: “By June, it was becoming clear that people were being admitted to hospital for non-Covid reasons who had tested positive many weeks before.
“Consequently, the NHS revised its situation report to accommodate this.”
https://www.thesun.co.uk/news/uknews/12459291/coronavirus-hospital-admissions-stats-overcount/
Here, it seems that PHE regularly looks for people on the NHS database who have ever tested positive, and simply checks to see if they are still alive or not. PHE does not appear to consider how long ago the COVID test result was, nor whether the person has been successfully treated in hospital and discharged to the community. Anyone who has tested COVID positive but subsequently died at a later date of any cause will be included on the PHE COVID death figures.
By this PHE definition, no one with COVID in England is allowed to ever recover from their illness. A patient who has tested positive, but successfully treated and discharged from hospital, will still be counted as a COVID death even if they had a heart attack or were run over by a bus three months later.
A positive test result shows you may have antibodies from an infection with the virus that causes COVID-19. However, there is a chance a positive result means that you have antibodies from an infection with a virus from the same family of viruses (called coronaviruses), such as the one that causes the common cold.
Regardless of whether you test positive or negative, the results do not confirm whether or not you are able to spread the virus that causes COVID-19.
https://www.cdc.gov/coronavirus/2019-ncov/testing/serology-overview.html