Professor Sucharit Bhakdi, one of the first medical experts to speak out against the Covid hysteria, is being prosecuted in Germany. Please see the resources below for more information.
Medical Experts
We collect information for this site from official data, mainstream sources and world-renowned experts.
Browse the articles related to this topic below.
Join our community on Guilded.
Professor Retsef Levi is an MIT Expert in Analytics, Risk Management, Health Systems, Food & Agriculture Systems, Manufacturing & Supply Chain Management.
The evidence is mounting and indisputable that MRNA vaccines cause serious harm including death, especially among young people.
…This is clearly the most failing medical product in the history of medical products, both in terms of efficacy and safety, And we need to investigate. How did we end up in a situation that it’s also the most profitable medical product in the history of medical products?
Nearly half of Americans believe Covid vaccines have probably caused a significant number of unexplained deaths, according to a Rasmussen Reports survey last week. In December, Rasmussen reported that a near equal proportion worry that Covid vaccines may have major side effects (57%) as believe they are effective (56%).
People can hold both views at the same time. But the self-professed expert class and many who call themselves journalists dismiss anyone who questions their Covid vaccine orthodoxy as an “anti-vaxxer”—a label as sneering as “climate denier.”But surveys show that most Americans, including those who didn’t get Covid shots, don’t distrust vaccines in general. Public views on Covid vaccines are more complicated because they are new and haven’t been thoroughly studied. The experts are responsible for vaccine skepticism because they aren’t honest about the potential risks.
Many doctors, in the UK and internationally, have become increasingly concerned about the safety profile of Covid-19 vaccines and the continued rollout of these products to the public, including pregnant women and children. Several doctors in DFPUK have submitted multiple Yellow Card reports of adverse events to the MHRA, and have signed letters to the JCVI, MHRA, the RCOG, Prime Minister and others to express their concerns, but have seen little or no response or action taken.
Advocates for harsh Covid measures are finally waking up to what they have done.
The underreported story of the entire pandemic is excess deaths — not from Covid, but from other health conditions which were so brutally pushed to one side. There have been huge rises in the number of people dying from causes unrelated to the virus, accelerating throughout the year and showing no signs of slowing down.
The World Health Organization amplified false Chinese statements about COVID-19 initially, while it dragging its feet on declaring an international emergency. Pandemic experts here clung to flu epidemic plans too, ignoring observable COVID-19 successes in East Asia and so ruling out any similar possibility of test-and-trace containment in the UK from the off.
Most public health experts then pivoted to being extremely pro-lockdown, but stuck rigidly to this even as the context, and so the costs and benefits of restrictions, changed with the vaccines and omicron.
Epidemiologists proved especially stubborn. Their modelling usually ignored the role of voluntary behavioural change entirely, so erred on the side of assuming catastrophic public health outcomes absent government mandates and restrictions. Hence, Freedom Day was dubbed “criminal” by scientists, while the government’s scientific advisers called for more restrictions last Christmas. Both proved wrong in retrospect.
Arguments to vaccinate children as young as five against Covid are ‘scientifically weak’, British experts claimed today after the US moved closer to jabbing infants.
…Professor David Livermore, a medical microbiologist at the University of East Anglia told MailOnline: ‘Vaccinating children to protect adults via herd immunity is ethically dubious and is scientifically weak.’
…Professor Russell Viner, a pediatrician and member of the UK Government’s scientific advisory group SAGE, said it was crucial the UK does not ‘rush to a decision’ in the wake of the announcement in the US.
Why haven’t lockdowns worked? There are broadly two types of respiratory virus. There are those that spread person to person – like measles – in a continuous chain of transmission, uninterrupted by season and with every susceptible contact falling ill. Then there are those we do not understand so well, like influenza, which are much more complex. Instead of the simplistic close contact model, which assumes Covid spreads like measles, we should perhaps consider an alternative more sophisticated model based on influenza. The influenza virus model is unusual – it is predicated on the majority being exposed to a particular airborne virus but, oddly, only a minority appear to be susceptible to each year’s variant. To complicate matters further, influenza can also spread person to person.
Riccardo Bosi interviews health professionals about censorship. Featuring Professor Dolores Cahill and Ros Nealon-Cook
https://www.facebook.com/australiaoneparty/videos/430638731822806
Backup mirrors:
Professor Sucharit Bhakdi: “You are now witnessing the greatest crime that England has ever committed in its history.”
Professor Sunetra Gupta of Oxford University explains herd immunity, highlighting critical details about both the concept and its relevance to the COVID-19 pandemic that are often overlooked in public discussion.
The development of immunity through natural infection is a common feature of many pathogens, and we now know that COVID-19 does not have any tricks up its sleeve to prevent this from happening. If it did, it would have posed a serious problem for the development of a vaccine.
That being said, COVID-19 belongs to a family of viruses that do not typically confer lifelong immunity against infection. Most of us have never heard of the other four ‘seasonal’ coronaviruses that are currently circulating in our communities. And yet, surveys indicate that at least 3% of the population is infected by any one of these corona cousins during the winter months each year. These viruses can – and do – cause deaths in high-risk groups or require them to receive ICU care or ventilator support. Hence, it is not necessarily true that they are intrinsically milder than the novel COVID-19 virus. And like the COVID-19 virus, the other coronas are much less virulent in the healthy elderly and younger people than influenza.
One important reason why these corona cousins do not kill large numbers of people is that, even though we lose immunity and can be reinfected, there is always a sufficient proportion of immune people within the population to keep the risk of infection low for those who might die upon contracting it. Also, all of the coronaviruses in circulation — including COVID-19 — have some features in common, which means that getting one coronavirus will probably offer some protection against the others. This is becoming increasingly clear from work in many labs, including my lab in Oxford. It is against the background of acquired immunity to COVID-19 itself, as well as its close relations, that the new virus has to operate.
It is misleading to speak of “reaching” herd immunity. Herd immunity is a continuous variable that increases as people become immune and decreases as they lose immunity or die. There is a threshold of herd immunity at which the rate of new infections begins to decrease. We do not yet have a clear idea of what this threshold is for COVID-19 as the transmission landscape includes people who are susceptible to it, people who have built up immunity to it, and people who have immunity to other coronaviruses.
Unfortunately, we do not have a good way of telling how many people have been exposed to the new virus, nor how many people were resistant to begin with. We can test for antibodies but, as with other coronaviruses, COVID-19 antibody levels decline after recovery, and some people do not make them at all. Thus, antibody levels will not answer this question. More and more evidence is accumulating that other arms of immunity, like T cells, play an important role.
Indications of the herd immunity threshold having been reached in a given location are visible in the time signatures of epidemics where death and infection curves tend to either “bend” in the absence of intervention or to stay down when interventions are relaxed (in comparison with other locations where the opposite happened). Unfortunately, we do not know how far (or close) we are to that threshold in most parts of the world. This means that we need to make public health decisions based only on limited information and do so in a constantly changing environment.
Focused Protection was initially proposed as a solution for how we could proceed in the face of such uncertainty and it remains relevant now. It suggests that we exploit the fact that COVID-19 does not cause much harm to the large majority of the population and allow those individuals to resume their normal lives, while shielding those who are vulnerable to severe disease and death. We have good information about who falls into these groups and the availability of vaccines, which offer excellent protection for vulnerable populations and guard against hospitalisable illness, provide us with the ideal setting in which to implement such a plan.
Sunetra Gupta is Professor of Theoretical Epidemiology in the Department of Zoology, University of Oxford and a member of Collateral Global’s Scientific Advisory Board.
By Professor Sunetra Gupta
28 May 2021
Backup mirrors:
Dr. Clare Craig points out an error by vaccines minister Nadhim Zahawi about what 60% vaccine efficacy means.
- If vaccines have 60% efficacy that does not mean that 60% cannot be infected.
- It means that if 90% of unvaccinated household contacts don’t catch it from index case, then if they were vaccinated that rises to 96%.
- Around 10% of close contacts catch it from an index case. (Source: Public Health England Technical Briefing 15)
- A vaccine with hypothetical 60% efficacy would reduce the proportion who caught it by 60% – to 4%.
- 90% would not catch it in either instance.
- 4% were protected thanks to vaccination.
Here is statement from Dr. Malcolm Kendrick which deserves to be archived in full. Links to the to original post and archive can be found below.
Thank you to the many people who have e-mailed me recently and asked if I have been silenced. I have not. I have had letters from Public Health England and the General Medical Council, informing me that I was under investigation for daring to question anything about COVID19, particularly vaccines.
The good news is the investigations ended up nowhere, and were closed down. I have also had irate phone calls from doctors, telling me that I must not question vaccination and suchlike. This has been somewhat wearing and has caused me to remain silent for a while and think about things.
However, I do know how to play the medical regulations game. Don’t make a statement you cannot reference from a peer-reviewed journal. Don’t give direct advice to people over the internet. Provide facts, and do not make statements such as ‘vaccines are killing thousands of people.’ Or suchlike.
Not that I ever would. My self-appointed role within the COVID19 mayhem, was to search for the truth – as far as it could be found – and to attempt to provide useful information for those who wish to read my blog.
The main reason for prolonged silence, and introspection, is that I am not sure I can find the truth. I do not know if it can be found anymore. Today I am unsure what represents a fact, and what has simply been made up. A sad and scary state of affairs.
This is not just true of the mainstream and the mainstream media, which has simply decided to parrot all Government and WHO statements without any critical engagement…or thought. For example, the BBC intones that ‘In the last day, fifty people died within twenty-eight days of a positive COVID19 test…’ Or a hundred, or six. What the hell is this supposed to mean? It means nothing, it is the very definition of scientific meaninglessness.
Especially when it seems that very nearly a half of those admitted to hospital with COVID19 were not admitted to hospital with COVID19. They were admitted with something else entirely, then had a positive test whilst in hospital. In short, they were not admitted to hospital with COVID19, and almost certainly did not die of COVID19. They died with a positive COVID19 test. With, not of.
But the misinformation is equally a problem for those on the other side. Claims are made for the benefits of Ivermectin and hydroxychloroquine that simply do not stand up to scrutiny. Yes, I believe both drugs may provide some benefit, but not the claimed 90% reduction in deaths that I have seen trumpeted.
So, I have given up on COVID19. It is a complete mess, and I feel that, without being certain of the ground under my feet, I have nothing to contribute. I too am in danger of starting to make statements that are not true.
However, before leaving the area entirely, I would like to make clear some of the things I currently believe to be true, and what I do not believe to be true. If this is of any assistance to anyone. Very little is referenced, because I can very easily find a contradictory reference to any reference I provide. For each fact, there is an equal and opposite fact.
1: SARS-CoV2 exists
Many people have stated, probably correctly, that the SARS-CoV2 virus has never been fully isolated. Whatever exactly that means. Have Koch’s postulates been met? [see a bit later on] I think for viruses, Koch’s postulates are very rarely, if ever, met. Does it matter, not really.
Despite this gap I believe that SARS-CoV2 truly is a ‘new’ virus that did not exist before. So, it must have mutated somewhere, or been mutated somewhere, from another coronavirus… probably. Although it seems that SARS-CoV2 does not mutate. Instead, it creates variants which, somehow or other, is a completely different process to a mutation! I have found that language in this area means little, and words are simply twisted to suit a particular narrative.
I feel it is most likely this mutation occurred within a laboratory in Wuhan during gain of function research. But I don’t suppose we will ever know. It seems unlikely to be something that the Chinese authorities are ever going to admit… ever. As a general rule, the more fervently, and angrily, the Chinese state denies something – the more likely it is to be true.
This is a special case of a general rule that I modestly call the ‘Kendrick reverse meaning law.’ Which developed from P.G. Wodehouse’s observation that ‘When an Englishman says ‘trust me’ it is time to start counting the spoons.’
This reverse meaning was seen clearly when Matt Hancock (UK Health Secretary at the time) stated that ‘Right from the start we’ve tried to throw a ring of steel around our care homes.’ Which actually meant that ‘Right from the start we threw care homes under a bus.’ Unless, what he actually meant was that the ring of steel was put up to stop care home residents escaping. ‘Halt, who goes there….’ Sound of heavy machine gun fire, whistles screeching, attack dogs baying at the leash. ‘Go for the Zimmer frames, that should bring them down.’
2: SARS-CoV2 is generally more deadly than influenza
Of course, SARS-CoV2 is most certainly not deadlier than the influenza epidemic of 1918-19. Which is estimated to have wiped out 2% of the entire world’s population. It is probably not more deadly than the 1957 epidemic, or the 1967 influenza epidemic. But it seems more deadly than anything in the last forty years, or so. So, a bit more deadly than most influenzas that sweep through humanity every year, or so. Give or take.
Currently, SARS-CoV2 is reckoned to have killed four and half million people across the Globe. Which is 0.07% of the world’s population. However, there is an immediate problem here. With influenza, we count for one year, then start again the next year. With COVID19 we have just kept on counting, adding this year figures to last years, and so on!
Eventually, therefore, assuming COVID19 comes and goes like the flu, and we just keep on counting without end, it will end up killing a hundred million. Making it the deadliest virus ever. Far worse than any influenza? At the current rate this will take another thirty years, or so. Within one thousand six hundred and sixty-six years it will have killed everyone. Of course, there will have been a few billion replacement humans created during that time.
What is far more important is to know the infection fatality rate (IFR)? That is, what percentage of those infected with SARS-CoV2 will die? This, I am afraid, we are never going to know, as the definition of what the word ‘infected’ means has flipped this way and that and can never be pinned down.
Does it mean a positive test? Does it mean a positive test plus symptoms? [Which used to be called a ‘case’] Does it mean something else. What does infected actually mean…
Here, I defer to the Master – Lewis Carroll:
‘When I use a word,” Humpty Dumpty said in rather a scornful tone, “it means just what I choose it to mean — neither more nor less.”
“The question is,” said Alice, “whether you can make words mean so many different things.”
“The question is,” said Humpty Dumpty, “which is to be master – – that’s all.”
Accepting that no-one will define what COVID19 infection actually means, I believe the infection fatality rate is, (using previous used definitions) settling at around 0.15%. At least it was last time I looked. This was never enough to justify the panicked actions that have taken place around the globe. Never.
3: The figures make no sense – and never will
One of the central problems here, form which all other problems flow, is that the PCR (polymerase chain reaction) test is the test against which the PCR test itself is tested. We have nothing better. So, we are completely reliant on it being accurate. However, we cannot know how accurate it truly is, because there is no test against which to compare it.
I mentioned Koch’s postulates earlier. These are the tests which can prove if a ‘micro-organism’ is actually causing the disease. The ultimate gold standard:
The microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms. The microorganism must be isolated from a diseased organism and grown in pure culture. The cultured microorganism should cause disease when introduced into a healthy organism. The microorganism must be re-isolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent. And good luck with all of that. The truth is that these postulates can work for bacteria, but not really for viruses. Because it is very difficult to meet them. I am not sure if they have ever been truly met for any virus.
On the matter of finding out if the virus is truly present, in anyone diagnosed with COVID19, here is a letter that was published in the BMJ in October last year
‘We are told that the virus is everywhere – in the air, in our breath, on fomites, trapped in masks – yet public health authorities seem not to be in possession of any cultivable clinical samples of the offending pathogen.
In March 2020, the World Health Organisation instructed authorities not to look for a virus but to rely instead on a genome test, the RT-PCR, which is not specific for SARS-CoV-2 (1) (2).
A Freedom of Information request to Public Health England about cultivable clinical samples or direct evidence of viral isolation has no information and refers to the proxy RT-PCR test, quoting Eurosurveillance (3).
Eurosurveillance states: “Virus detection by reverse transcription-PCR (RT-PCR) from respiratory samples is widely used to diagnose and monitor SARS-CoV-2 infection and, increasingly, to infer infectivity of an individual. However, RT-PCR does not distinguish between infectious and non-infectious virus. Propagating virus from clinical samples confirms the presence of infectious virus but is not widely available (and) requires biosafety level 3 facilities” (4).
The CDC admits that, “no quantified virus isolates of the 2019-nCoV are currently available”, and used a genetically modified human lung alveolar adenocarcinoma cell culture to, “mimic clinical specimen”(5).
It appears, therefore, that we have public health bodies without clinical samples, a test which is non-specific and does not distinguish between infectivity and non-infectivity, a requirement for biosafety level 3 facilities to even look for a virus, yet we are led to believe that it is up all our noses.
So, where is the virus?’
(1) https://www.who.int/publications/i/item/10665-331501
(2) https://www.bmj.com/content/369/bmj.m2420/rr-5
(3) https://www.whatdotheyknow.com/request/679566/response/1625332/attach/ht…
(4) https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.32…
(5) https://www.fda.gov/media/134922/download 1
After reading this, do I still think SARS-CoV2 exists? Yes, I do. I firmly believe that I watched people dying of it, from it. They died in a way I have never seen people do so before, and I have seen a lot of people die. They seemed quite well, then suddenly their oxygen sats dropped like a stone – they still seemed okay otherwise – then they died. The end.
Very strange, and rather disturbing. I started slipping an oxygen saturation monitor onto my finger from time to time. Just in case. 99% is my average reading, if you are interested. It never dropped.
However, getting back to the testing. If you truly want to confirm the presence of a virus in a sample, you need to send it to biosafety level 3 facilities to isolate it, grow it (not really the correct word for a virus), and suchlike. This is never done in the clinical setting.
You could argue that if you wait for antibodies to develop, you can ‘prove’ that someone was infected, or not, and thus work out how accurate the PCR test has been retrospectively. Perhaps…
I speak as someone who needed seven Hepatitis B vaccinations before I produced any detectable antibodies. Did I have immunity after the first six, or not? Am I someone who simply does not make many antibodies, but still have immunity through other mechanisms? Do others simply not produce antibodies, or their level drops so fast, that they effectively disappear?
Yes, serological testing (looking for antibodies), has its own very significant problems.
‘Serological tests for SARS-CoV-2 have accuracy issues that warrant attention. They measure specific antibody responses which may take some weeks to develop after disease onset reducing the sensitivity of the assay. If blood samples were collected during the early stage of the infection, they may produce false negative results. They do not directly detect the presence of the virus. Further, antibodies may be present when SARS-CoV-2 is no longer present giving false positive case diagnosis.’ 2
In reality, we are relying on a PCR test to diagnose SARS-CoV2 infection, the accuracy of which is entirely dependent on believing that the test is accurate. Yes, that is the route to madness.
At present, in the UK, we are doing about one million tests a day 3.
We are getting about thirty thousand ‘positive’ results. Or, about 3% positive. How many of these are truly positive? Well, you can take a wild guess on that one. At one point, the CDC stated that 30% of the PCR tests were false positives. A ‘false positive’ means that test says you have the disease, when you do not. [A false negative informs you that you do not have the disease, when you do] 4.
The thirty per cent cannot be the case currently, because that would mean if you did one million tests, you would get more than three hundred thousand false positives. Instead we are getting thirty thousand, which means that it is impossible for the false positive rate to be higher than three per cent.
So, what is the true rate? Well, if is three percent, then virtually every single positive test is a false positive test. [Three per cent of one million is thirty thousand] Which would mean that no-one in the UK currently has COVID19, and everything we are doing is completely pointless. It also means that people admitted to hospital with COVID19 do not have the disease, they are suffering from, and dying from, something else with a false positive COVID19 false test stamped on their forehead.
Is it possible that no-one actually is infected with SARS-CoV2? Well, it is certainly not impossible. Here is a graph of overall mortality (risk of dying of anything) from England. These figures, unlike most others, are pretty much fully reliable. Someone is either dead, or they are not. It is a difficult thing to get wrong, or manipulate. There can be some delay in registering a death, but this is not normally a major issue.
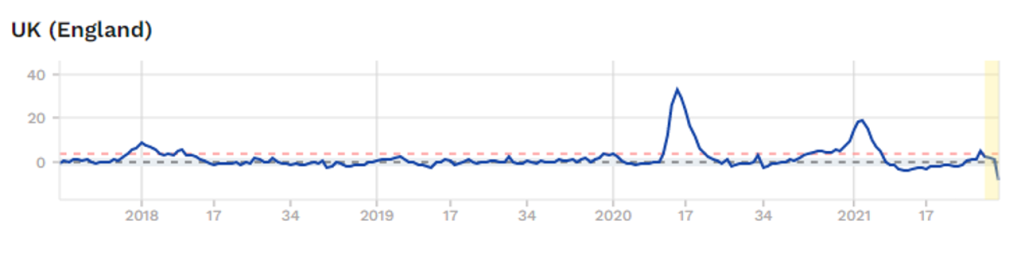
The graph starts in last quarter 2017. As you can see, a spike in overall mortality in Spring 2020, A spike in Winter 2020/21. Currently, no excess mortality at all. So, if COVID19 is infecting hundreds of thousands of people each week, it is not showing up as any excess deaths… at all 5.
Does this mean that COVID19 has gone, and we are rushing around panicking about false positive tests? Or is it still here? Still here I think… but who knows… who knows.
This is the main reason I have given up. I just don’t know what to believe – apart from overall mortality figures. The figures are spun and massage, twisted and mangled.
Another reason why I have given up trying to make any sense of COVID19 is the enormous differences in overall mortality seen in countries that are virtually identical in life expectancy, healthcare systems, actions taken against COVID19 etc. etc.
Afters studying the figures from England, I looked at the figures from Northern Ireland.
Both countries [yes, Northern Ireland is not actually a separate country, it is part of the UK] did almost exactly the same things when it came to COVID19. They both have the National Health Service, they are as close to each other as can be – in terms of COVID19, and most other things. Here is the graph of overall morality for Northern Ireland.
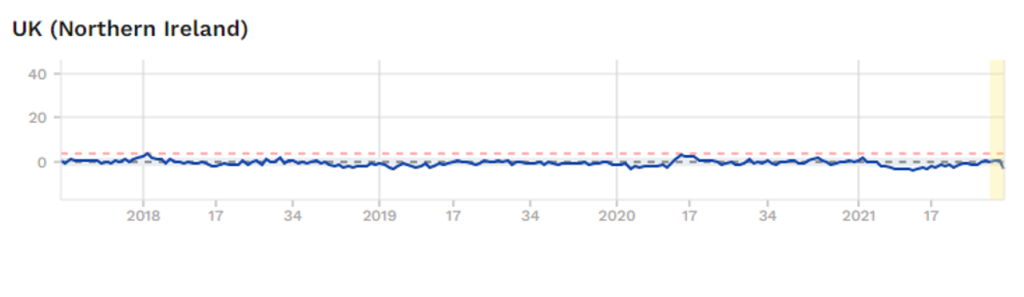
Which means that something very dramatic happened in England, with regard to COVID19? Yet nothing happened in Northern Ireland. This, to me, is fascinating, although I cannot explain it. However, I know that if you were able explain why these two graphs are so weirdly different, you will be unearthing some critical truths with regard to COVID19.
Of course, no-one is remotely interested in such anomalies. Instead, they point to a country like Norway and say – ‘Look how well they did with their rapid lockdown, and preventing people crossing the border’. No-one points to Northern Ireland and says, ‘look how well they did with all their….’ All their what? All their doing exactly the same as England.
Yes, Northern Ireland does not fit with the approved narrative, so it is ignored. Anything that does not fit with the mask wearing, social isolating, vaccination will save the world narrative is simply ignored.
Or it is shouted down or censored by the self-appointed Fact-checkers. Those mighty intellects who can determine what is true, and what is not. It was thoughtful of them to descend from Mount Olympus to mingle amongst feeble minded humanity and tell us what we should, and should not, be thinking. We must all be eternally grateful that the ‘Truth Gods’ now live amongst us, to firmly inform us all what, and how, we should be thinking. And shut us down if we veer from the official narrative.
Anyway, faced with a situation where there are almost no facts that can be relied upon, from anywhere, I have officially removed myself from all discussions on the matter of COVID19.
Instead, I shall return to other areas where, whilst the truth is constantly battered and bruised, and lying in a bruised heap the corner, it is still breathing … just about alive. Sometimes it is capable of weakly raising its head and whispering quietly into my ear. I shall let you know what it says.
1: https://www.bmj.com/content/370/bmj.m3379/rr-2
2: https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-021-01689-3
3: https://coronavirus.data.gov.uk/?_ga=2.38943459.111756282.1590603430-1775824629.1590603430
4: https://www.bmj.com/content/373/bmj.n1411/rr
5: https://www.euromomo.eu/graphs-and-maps/
https://drmalcolmkendrick.org/2021/09/03/i-have-not-been-silenced/
Vaccines typically do not outperform natural immunity, so it should come as no surprise that Covid vaccines do not offer long-term protection against infection. At the same time, we can be confident that they will continue to work well to prevent severe clinical outcomes. The role of these vaccines is to offer protection to the clinically vulnerable; to foist them upon those who are at negligible risk in the hope of augmenting herd immunity is illogical…
Will boosters achieve what two doses could not? For those who are extremely vulnerable and show no evidence of mounting a significant immune response after two doses, it is entirely reasonable to attempt a third dose.
But it can be to no-one else’s individual gain to submit to a third jab, having already reduced the risk of severe disease (which was very small in the first place for most) by receiving two inoculations. For there to be the collective benefit of herd immunity, the booster would have to provide life-long protection against infection – unless we are willing to accept repeated mass vaccination into the foreseeable future. Aside from being a colossal diversion of limited resources, that would open the door to a permanent state of lockdown as we lurch from one booster campaign to the next.
We write as concerned doctors, nurses, and other allied healthcare professionals with no vested interest in doing so. To the contrary, we face personal risk in relation to our employment for doing so and / or the risk of being personally “smeared” by those who inevitably will not like us speaking out.
Categories
Dr. Tess Lawrie Interview – Oracle Films
Dr. Tess Lawrie is a world-class researcher and consultant to the World Health Organisation. Her biggest clients happen to be those who are involved in the suppression of repurposed drugs. She has decided to speak out in protest against the current medical establishment at considerable personal risk.
She co-founded the BiRD Group; an international consortium of experts dedicated to the transparent and accurate scientific research of Ivermectin, with particular emphasis on the treatment and prevention of Covid-19.
Dr Sam White is a GP in the UK. He was recently suspended by the NHS for speaking out about informed consent, the safety of the vaccine and other safe and effective alternative treatments.
He is now running a campaign to promote his concerns about the vaccine and the plan to vaccinate children.
Categories
Contagion Myth – Session 1, Dr. Tom Cowan
Some good news and some troubling news, from Professor Sucharit Bhakdi, M.D.
Oracle Films recently produced an interview with Professor Sucharit Bhakdi in collaboration with Oval Media in Germany, for an upcoming documentary.
As an aside to the interview, Dr. Bhakdi emphasised the urgent need to share the following information that has emerged from new scientific literature.
PLEASE take the time to process this presentation. Dr. Bhakdi explains clearly, based on new scientific evidence, why he believes:
* Your immune system is your best defence against SARS-CoV-2, and indeed all coronaviruses. If you have been infected, even if you experienced no symptoms at all, you are immune to all variants.
* We have already reached herd immunity.
* There is no scientific reason to vaccinate against SARS-CoV-2. There is simply no benefit and the rollout must be stopped.
Scientific literature references for Dr. Bhakdi’s presentation:
- https://www.sciencedirect.com/science/article/pii/S2352396421002036
- https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0249499
- https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab465/6279075
- https://doi.org/10.1016/j.cell.2021.06.005
Update: On 17 July 2021, Dr. Geert Vanden Bossche posted a response to Dr. Bhakdi’s conclusions. Both agree that mass vaccination should halt but differ on the dangers of variants and whether herd immunity has been reached.
The Associated Press recently ran a story they said debunked the dissenting Covid concerns of pathologist, Dr. Roger Hodkinson. In their article titled, “Pathologist falsely claims COVID-19 is a hoax, no worse than the flu,” they misrepresented several of Dr. Hodkinson’s statements. The also wrote specifically saying they were planning to debunk him, not understand what he meant. Dr Hodkinson is a medical specialist in pathology and graduate of Cambridge University, UK. He is a Fellow of the College of American Pathologists and the Royal College of Physicians and Surgeons of Canada. He was previously the President of the Alberta Society of Laboratory Physicians, an Assistant Professor in the Faculty of Medicine at the University of Alberta, and CEO of a large community based medical laboratory with a full menu of testing for infectious disease and virology. He is currently the Chairman of an American biotechnology company active in DNA sequencing.