Dr. John Campbell is an internet sensation, giving facts & data to help us navigate healthcare in the present day. The interview covers John’s development, work, rise to fame & what he would do to help get healthcare back in shape.
Hydroxychloroquine
Browse the articles related to this topic below.
Join our community on Guilded.
In an exclusive and explosive one-hour interview with Veronika Kyrylenko of The New American, pioneering mRNA scientist Dr. Robert Malone explains the intensely corrupt workings of the government regulatory bodies that have mismanaged the pandemic, discusses the problems with the vaccine program and delves into potentially explosive and game-changing revelations about the shady origins of the Covid-19 pandemic in Wuhan, China.
Here is statement from Dr. Malcolm Kendrick which deserves to be archived in full. Links to the to original post and archive can be found below.
Thank you to the many people who have e-mailed me recently and asked if I have been silenced. I have not. I have had letters from Public Health England and the General Medical Council, informing me that I was under investigation for daring to question anything about COVID19, particularly vaccines.
The good news is the investigations ended up nowhere, and were closed down. I have also had irate phone calls from doctors, telling me that I must not question vaccination and suchlike. This has been somewhat wearing and has caused me to remain silent for a while and think about things.
However, I do know how to play the medical regulations game. Don’t make a statement you cannot reference from a peer-reviewed journal. Don’t give direct advice to people over the internet. Provide facts, and do not make statements such as ‘vaccines are killing thousands of people.’ Or suchlike.
Not that I ever would. My self-appointed role within the COVID19 mayhem, was to search for the truth – as far as it could be found – and to attempt to provide useful information for those who wish to read my blog.
The main reason for prolonged silence, and introspection, is that I am not sure I can find the truth. I do not know if it can be found anymore. Today I am unsure what represents a fact, and what has simply been made up. A sad and scary state of affairs.
This is not just true of the mainstream and the mainstream media, which has simply decided to parrot all Government and WHO statements without any critical engagement…or thought. For example, the BBC intones that ‘In the last day, fifty people died within twenty-eight days of a positive COVID19 test…’ Or a hundred, or six. What the hell is this supposed to mean? It means nothing, it is the very definition of scientific meaninglessness.
Especially when it seems that very nearly a half of those admitted to hospital with COVID19 were not admitted to hospital with COVID19. They were admitted with something else entirely, then had a positive test whilst in hospital. In short, they were not admitted to hospital with COVID19, and almost certainly did not die of COVID19. They died with a positive COVID19 test. With, not of.
But the misinformation is equally a problem for those on the other side. Claims are made for the benefits of Ivermectin and hydroxychloroquine that simply do not stand up to scrutiny. Yes, I believe both drugs may provide some benefit, but not the claimed 90% reduction in deaths that I have seen trumpeted.
So, I have given up on COVID19. It is a complete mess, and I feel that, without being certain of the ground under my feet, I have nothing to contribute. I too am in danger of starting to make statements that are not true.
However, before leaving the area entirely, I would like to make clear some of the things I currently believe to be true, and what I do not believe to be true. If this is of any assistance to anyone. Very little is referenced, because I can very easily find a contradictory reference to any reference I provide. For each fact, there is an equal and opposite fact.
1: SARS-CoV2 exists
Many people have stated, probably correctly, that the SARS-CoV2 virus has never been fully isolated. Whatever exactly that means. Have Koch’s postulates been met? [see a bit later on] I think for viruses, Koch’s postulates are very rarely, if ever, met. Does it matter, not really.
Despite this gap I believe that SARS-CoV2 truly is a ‘new’ virus that did not exist before. So, it must have mutated somewhere, or been mutated somewhere, from another coronavirus… probably. Although it seems that SARS-CoV2 does not mutate. Instead, it creates variants which, somehow or other, is a completely different process to a mutation! I have found that language in this area means little, and words are simply twisted to suit a particular narrative.
I feel it is most likely this mutation occurred within a laboratory in Wuhan during gain of function research. But I don’t suppose we will ever know. It seems unlikely to be something that the Chinese authorities are ever going to admit… ever. As a general rule, the more fervently, and angrily, the Chinese state denies something – the more likely it is to be true.
This is a special case of a general rule that I modestly call the ‘Kendrick reverse meaning law.’ Which developed from P.G. Wodehouse’s observation that ‘When an Englishman says ‘trust me’ it is time to start counting the spoons.’
This reverse meaning was seen clearly when Matt Hancock (UK Health Secretary at the time) stated that ‘Right from the start we’ve tried to throw a ring of steel around our care homes.’ Which actually meant that ‘Right from the start we threw care homes under a bus.’ Unless, what he actually meant was that the ring of steel was put up to stop care home residents escaping. ‘Halt, who goes there….’ Sound of heavy machine gun fire, whistles screeching, attack dogs baying at the leash. ‘Go for the Zimmer frames, that should bring them down.’
2: SARS-CoV2 is generally more deadly than influenza
Of course, SARS-CoV2 is most certainly not deadlier than the influenza epidemic of 1918-19. Which is estimated to have wiped out 2% of the entire world’s population. It is probably not more deadly than the 1957 epidemic, or the 1967 influenza epidemic. But it seems more deadly than anything in the last forty years, or so. So, a bit more deadly than most influenzas that sweep through humanity every year, or so. Give or take.
Currently, SARS-CoV2 is reckoned to have killed four and half million people across the Globe. Which is 0.07% of the world’s population. However, there is an immediate problem here. With influenza, we count for one year, then start again the next year. With COVID19 we have just kept on counting, adding this year figures to last years, and so on!
Eventually, therefore, assuming COVID19 comes and goes like the flu, and we just keep on counting without end, it will end up killing a hundred million. Making it the deadliest virus ever. Far worse than any influenza? At the current rate this will take another thirty years, or so. Within one thousand six hundred and sixty-six years it will have killed everyone. Of course, there will have been a few billion replacement humans created during that time.
What is far more important is to know the infection fatality rate (IFR)? That is, what percentage of those infected with SARS-CoV2 will die? This, I am afraid, we are never going to know, as the definition of what the word ‘infected’ means has flipped this way and that and can never be pinned down.
Does it mean a positive test? Does it mean a positive test plus symptoms? [Which used to be called a ‘case’] Does it mean something else. What does infected actually mean…
Here, I defer to the Master – Lewis Carroll:
‘When I use a word,” Humpty Dumpty said in rather a scornful tone, “it means just what I choose it to mean — neither more nor less.”
“The question is,” said Alice, “whether you can make words mean so many different things.”
“The question is,” said Humpty Dumpty, “which is to be master – – that’s all.”
Accepting that no-one will define what COVID19 infection actually means, I believe the infection fatality rate is, (using previous used definitions) settling at around 0.15%. At least it was last time I looked. This was never enough to justify the panicked actions that have taken place around the globe. Never.
3: The figures make no sense – and never will
One of the central problems here, form which all other problems flow, is that the PCR (polymerase chain reaction) test is the test against which the PCR test itself is tested. We have nothing better. So, we are completely reliant on it being accurate. However, we cannot know how accurate it truly is, because there is no test against which to compare it.
I mentioned Koch’s postulates earlier. These are the tests which can prove if a ‘micro-organism’ is actually causing the disease. The ultimate gold standard:
The microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms. The microorganism must be isolated from a diseased organism and grown in pure culture. The cultured microorganism should cause disease when introduced into a healthy organism. The microorganism must be re-isolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent. And good luck with all of that. The truth is that these postulates can work for bacteria, but not really for viruses. Because it is very difficult to meet them. I am not sure if they have ever been truly met for any virus.
On the matter of finding out if the virus is truly present, in anyone diagnosed with COVID19, here is a letter that was published in the BMJ in October last year
‘We are told that the virus is everywhere – in the air, in our breath, on fomites, trapped in masks – yet public health authorities seem not to be in possession of any cultivable clinical samples of the offending pathogen.
In March 2020, the World Health Organisation instructed authorities not to look for a virus but to rely instead on a genome test, the RT-PCR, which is not specific for SARS-CoV-2 (1) (2).
A Freedom of Information request to Public Health England about cultivable clinical samples or direct evidence of viral isolation has no information and refers to the proxy RT-PCR test, quoting Eurosurveillance (3).
Eurosurveillance states: “Virus detection by reverse transcription-PCR (RT-PCR) from respiratory samples is widely used to diagnose and monitor SARS-CoV-2 infection and, increasingly, to infer infectivity of an individual. However, RT-PCR does not distinguish between infectious and non-infectious virus. Propagating virus from clinical samples confirms the presence of infectious virus but is not widely available (and) requires biosafety level 3 facilities” (4).
The CDC admits that, “no quantified virus isolates of the 2019-nCoV are currently available”, and used a genetically modified human lung alveolar adenocarcinoma cell culture to, “mimic clinical specimen”(5).
It appears, therefore, that we have public health bodies without clinical samples, a test which is non-specific and does not distinguish between infectivity and non-infectivity, a requirement for biosafety level 3 facilities to even look for a virus, yet we are led to believe that it is up all our noses.
So, where is the virus?’
(1) https://www.who.int/publications/i/item/10665-331501
(2) https://www.bmj.com/content/369/bmj.m2420/rr-5
(3) https://www.whatdotheyknow.com/request/679566/response/1625332/attach/ht…
(4) https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.32…
(5) https://www.fda.gov/media/134922/download 1
After reading this, do I still think SARS-CoV2 exists? Yes, I do. I firmly believe that I watched people dying of it, from it. They died in a way I have never seen people do so before, and I have seen a lot of people die. They seemed quite well, then suddenly their oxygen sats dropped like a stone – they still seemed okay otherwise – then they died. The end.
Very strange, and rather disturbing. I started slipping an oxygen saturation monitor onto my finger from time to time. Just in case. 99% is my average reading, if you are interested. It never dropped.
However, getting back to the testing. If you truly want to confirm the presence of a virus in a sample, you need to send it to biosafety level 3 facilities to isolate it, grow it (not really the correct word for a virus), and suchlike. This is never done in the clinical setting.
You could argue that if you wait for antibodies to develop, you can ‘prove’ that someone was infected, or not, and thus work out how accurate the PCR test has been retrospectively. Perhaps…
I speak as someone who needed seven Hepatitis B vaccinations before I produced any detectable antibodies. Did I have immunity after the first six, or not? Am I someone who simply does not make many antibodies, but still have immunity through other mechanisms? Do others simply not produce antibodies, or their level drops so fast, that they effectively disappear?
Yes, serological testing (looking for antibodies), has its own very significant problems.
‘Serological tests for SARS-CoV-2 have accuracy issues that warrant attention. They measure specific antibody responses which may take some weeks to develop after disease onset reducing the sensitivity of the assay. If blood samples were collected during the early stage of the infection, they may produce false negative results. They do not directly detect the presence of the virus. Further, antibodies may be present when SARS-CoV-2 is no longer present giving false positive case diagnosis.’ 2
In reality, we are relying on a PCR test to diagnose SARS-CoV2 infection, the accuracy of which is entirely dependent on believing that the test is accurate. Yes, that is the route to madness.
At present, in the UK, we are doing about one million tests a day 3.
We are getting about thirty thousand ‘positive’ results. Or, about 3% positive. How many of these are truly positive? Well, you can take a wild guess on that one. At one point, the CDC stated that 30% of the PCR tests were false positives. A ‘false positive’ means that test says you have the disease, when you do not. [A false negative informs you that you do not have the disease, when you do] 4.
The thirty per cent cannot be the case currently, because that would mean if you did one million tests, you would get more than three hundred thousand false positives. Instead we are getting thirty thousand, which means that it is impossible for the false positive rate to be higher than three per cent.
So, what is the true rate? Well, if is three percent, then virtually every single positive test is a false positive test. [Three per cent of one million is thirty thousand] Which would mean that no-one in the UK currently has COVID19, and everything we are doing is completely pointless. It also means that people admitted to hospital with COVID19 do not have the disease, they are suffering from, and dying from, something else with a false positive COVID19 false test stamped on their forehead.
Is it possible that no-one actually is infected with SARS-CoV2? Well, it is certainly not impossible. Here is a graph of overall mortality (risk of dying of anything) from England. These figures, unlike most others, are pretty much fully reliable. Someone is either dead, or they are not. It is a difficult thing to get wrong, or manipulate. There can be some delay in registering a death, but this is not normally a major issue.
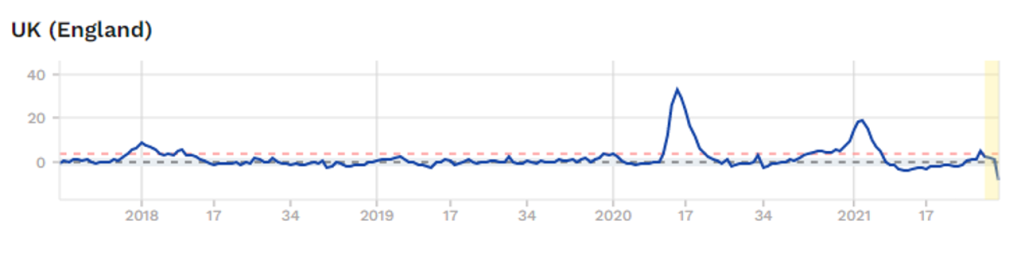
The graph starts in last quarter 2017. As you can see, a spike in overall mortality in Spring 2020, A spike in Winter 2020/21. Currently, no excess mortality at all. So, if COVID19 is infecting hundreds of thousands of people each week, it is not showing up as any excess deaths… at all 5.
Does this mean that COVID19 has gone, and we are rushing around panicking about false positive tests? Or is it still here? Still here I think… but who knows… who knows.
This is the main reason I have given up. I just don’t know what to believe – apart from overall mortality figures. The figures are spun and massage, twisted and mangled.
Another reason why I have given up trying to make any sense of COVID19 is the enormous differences in overall mortality seen in countries that are virtually identical in life expectancy, healthcare systems, actions taken against COVID19 etc. etc.
Afters studying the figures from England, I looked at the figures from Northern Ireland.
Both countries [yes, Northern Ireland is not actually a separate country, it is part of the UK] did almost exactly the same things when it came to COVID19. They both have the National Health Service, they are as close to each other as can be – in terms of COVID19, and most other things. Here is the graph of overall morality for Northern Ireland.
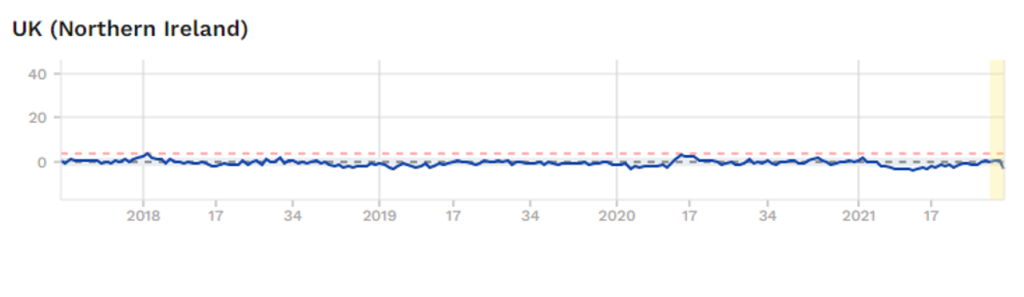
Which means that something very dramatic happened in England, with regard to COVID19? Yet nothing happened in Northern Ireland. This, to me, is fascinating, although I cannot explain it. However, I know that if you were able explain why these two graphs are so weirdly different, you will be unearthing some critical truths with regard to COVID19.
Of course, no-one is remotely interested in such anomalies. Instead, they point to a country like Norway and say – ‘Look how well they did with their rapid lockdown, and preventing people crossing the border’. No-one points to Northern Ireland and says, ‘look how well they did with all their….’ All their what? All their doing exactly the same as England.
Yes, Northern Ireland does not fit with the approved narrative, so it is ignored. Anything that does not fit with the mask wearing, social isolating, vaccination will save the world narrative is simply ignored.
Or it is shouted down or censored by the self-appointed Fact-checkers. Those mighty intellects who can determine what is true, and what is not. It was thoughtful of them to descend from Mount Olympus to mingle amongst feeble minded humanity and tell us what we should, and should not, be thinking. We must all be eternally grateful that the ‘Truth Gods’ now live amongst us, to firmly inform us all what, and how, we should be thinking. And shut us down if we veer from the official narrative.
Anyway, faced with a situation where there are almost no facts that can be relied upon, from anywhere, I have officially removed myself from all discussions on the matter of COVID19.
Instead, I shall return to other areas where, whilst the truth is constantly battered and bruised, and lying in a bruised heap the corner, it is still breathing … just about alive. Sometimes it is capable of weakly raising its head and whispering quietly into my ear. I shall let you know what it says.
1: https://www.bmj.com/content/370/bmj.m3379/rr-2
2: https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-021-01689-3
3: https://coronavirus.data.gov.uk/?_ga=2.38943459.111756282.1590603430-1775824629.1590603430
4: https://www.bmj.com/content/373/bmj.n1411/rr
5: https://www.euromomo.eu/graphs-and-maps/
https://drmalcolmkendrick.org/2021/09/03/i-have-not-been-silenced/
Dr Sam White is a GP in the UK. He was recently suspended by the NHS for speaking out about informed consent, the safety of the vaccine and other safe and effective alternative treatments.
He is now running a campaign to promote his concerns about the vaccine and the plan to vaccinate children.
University of Oxford scientists are trialling giving Ivermectin to over-50s with Covid symptoms to see if it can keep them out of hospital.
http://archive.today/2021.06.23-080235/https://www.bbc.com/news/health-57570377
Dr. Peter McCullough has been the world’s most prominent and vocal advocate for early outpatient treatment of SARS-CoV-2 (COVID-19) infection in order to prevent hospitalization and death. On May 19, 2021, I interviewed him about his efforts as a treating physician and researcher. From his unique vantage point, he has observed and documented a profoundly disturbing policy response to the pandemic—a policy response that may prove to be the greatest malpractice and malfeasance in the history of medicine and public health.”
Link to interview audio format released by Julian Charles of The Mind Renewed podcast.
Backup mirror:
Ivor Cummins aka the Fat Emperor – gives James the lowdown on why you can’t trust anything our governments tell us about Covid-19. If you want the facts on Coronavirus – how deadly is it? do lockdowns and masks work? how does it compare with previous pandemics? – you’ve come to the right place
Please support the Delingpod:
Mirror archives are available below if this video is removed from YouTube.
First COVID-19 outpatient study based on risk stratification and early antiviral treatment at the beginning of the disease.
Low-dose hydroxychloroquine combined with zinc and azithromycin was an effective therapeutic approach against COVID-19.
Significantly reduced hospitalisation rates in the treatment group.
Reduced mortality rates in the treatment group.
Hydroxychloroquine really works says Professor of Medicine Dr Peter McCullough, describing the treatment as “the most widely used therapeutic” to treat COVID-19 in the world.
“The chances that it doesn’t work are calculated to be one in 17 billion,” he told Sky News.
“There’s no controversy over whether or not hydroxychloroquine works. The controversy is on the public health approach to COVID-19.”
Mr McCullough said “the virus invades inside cells, so we have to use drugs that go inside the cell and work to reduce viral replication”.
“The drugs that work within the cell and actually reduce viral replication are hydroxychloroquine, Ivermectin, doxycycline and azithromycin”.
“Sadly, in the United States and I know in Australia this happens all the time, patients get no treatment whatsoever. They literally are told to stay at home until they are sick enough to go to the hospital”
“I think that honestly it’s atrocious.
“History will look back on that and think it was the worst way to handle a potentially fatal illness.”
https://web.archive.org/web/20201129025607/https://www.skynews.com.au/details/_6212859932001
- AIDS was a testing pandemic, just like COVID-19.
- Many of the excess deaths for COVID-19 were due to inappropriately high dosages of hydroxychloroquine during experimental study trials.
- High COVID-19 excess deaths stopped after the trials were ended.
- Professor Martin Landry, leader of the UK-based Recovery trial, may have made a mistake in proposing high dosage of hydroxychloroquine. It seems he confused it with diiodohydroxyquinoline, treatment for treatment of amoebiasis.
- The treatment caused the damage.
- The danger of over-treatment is everywhere because the industry wants to sell diseases.
- COVID-19 is a self-limiting disease.
- The data shows that COVID-19 has no more killing potential than the yearly flu.
- Masks and lockdowns are ridiculous and damaging the whole population.
- It’s a political thing and not a health problem.
- Remdesivir is an immunosuppressant and useless against COVID-19.
- You have to live with viruses and you can’t fight against them.
- There is no treatment against COVID-19.
- The treatment against COVID-19 is to rest, like the flu.
- The problem is testing. If you stop the test, you’ll see nothing.
- Lockdowns were an overreaction.
- Vaccines are probably not a solution. You’ll have to vaccinate everyone every year. It’s good businesses.
The aim of this study was to describe the outcomes of patients with coronavirus disease 2019 (COVID-19) in the outpatient setting after early treatment with zinc, low-dose hydroxychloroquine and azithromycin (triple therapy) dependent on risk stratification. This was a retrospective case series study in the general practice setting. A total of 141 COVID-19 patients with laboratory-confirmed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection in the year 2020 were included. The main outcome measures were risk-stratified treatment decision and rates of hospitalisation and all-cause death. A median of 4 days [interquartile range (IQR) 3-6 days; available for n = 66/141 patients] after the onset of symptoms, 141 patients (median age 58 years, IQR 40-67 years; 73.0% male) received a prescription for triple therapy for 5 days. Independent public reference data from 377 confirmed COVID-19 patients in the same community were used as untreated controls. Of 141 treated patients, 4 (2.8%) were hospitalised, which was significantly fewer (P < 0.001) compared with 58 (15.4%) of 377 untreated patients [odds ratio (OR) = 0.16, 95% confidence interval (CI) 0.06-0.5]. One patient (0.7%) in the treatment group died versus 13 patients (3.4%) in the untreated group (OR = 0.2, 95% CI 0.03-1.5; P = 0.12). No cardiac side effects were observed. Risk stratification-based treatment of COVID-19 outpatients as early as possible after symptom onset using triple therapy, including the combination of zinc with low-dose hydroxychloroquine, was associated with significantly fewer hospitalisations.
None of this, however, explains the 40 years of medical
misinformation and suppression of the pharmaceutical truth.
To have covered up the knowledge for four decades that
viruses could potentially be treated by antimicrobials required
extensive effort:
• Censorship. It is likely that some scientists were never
published again after authoring one paper on the antiviral benefits of CQ.
• Buying silence of news media. This is evident from the
blackout across the political news spectrum concerning
vaccine adverse effects. Pharmaceutical manufacturers
provide the most lucrative advertising for both written
and broadcast news programs.
• Misdirection. For years, pharmacology professors in
medical schools have perpetuated lies of omission.
• Lies by drug companies. Merck was caught publishing its
own “peer reviewed” journal to promote its drugs.54
• Regulatory capture. “Big Pharma” essentially owns the
FDA by being its biggest funder and employing more
than 58 percent of the FDA’s upper-level regulators and
administrators either before or after their tenure.55,56
• Research funding. Big Pharma is the major funder of
nearly all “independent” drug research, and there is no
incentive to research cheap/ less profitable solutions.
The COVID-19 pandemic is calling attention to the
potential for treating viral diseases with currently available
drugs, and exposing long-available but ignored research.
The implications of all this are very disturbing. Where have
the virologists been, and the CDC “experts” who claim to care
about influenza deaths? Has the burgeoning nearly trilliondollar vaccine industry been built at the expense of patients’
lives?
As professor of epidemiology at Yale School of Public Health, I have authored over 300 peer-reviewed publications and currently hold senior positions on the editorial boards of several leading journals. I am usually accustomed to advocating for positions within the mainstream of medicine, so have been flummoxed to find that, in the midst of a crisis, I am fighting for a treatment that the data fully support but which, for reasons having nothing to do with a correct understanding of the science, has been pushed to the sidelines. As a result, tens of thousands of patients with COVID-19 are dying unnecessarily. Fortunately, the situation can be reversed easily and quickly.
I am referring, of course, to the medication hydroxychloroquine. When this inexpensive oral medication is given very early in the course of illness, before the virus has had time to multiply beyond control, it has shown to be highly effective, especially when given in combination with the antibiotics azithromycin or doxycycline and the nutritional supplement zinc.
- As a result, tens of thousands of patients with COVID-19 are dying unnecessarily.
- An inexpensive and be highly effective treatment, especially when given early: Hydroxychloroquine in combination with the antibiotics azithromycin or doxycycline and zinc.
- The article, “Early Outpatient Treatment of Symptomatic, High-Risk COVID-19 Patients that Should be Ramped-Up Immediately as Key to the Pandemic Crisis” was published in the American Journal of Epidemiology (AJE). It analyzed five studies, demonstrating clear benefits and safety of this treatment.
- Other studies include:
- an additional 400 high-risk patients treated by Dr. Vladimir Zelenko, with zero deaths;
- four studies totaling almost 500 high-risk patients treated in nursing homes and clinics across the U.S., with no deaths;
- a controlled trial of more than 700 high-risk patients in Brazil, with significantly reduced risk of hospitalization and two deaths among 334 patients treated with hydroxychloroquine;
- and another study of 398 matched patients in France, also with significantly reduced hospitalization risk.
- “Natural experiments:” northern Brazil state of Pará used hydroxychloroquine to reduce deaths.
- Hydroxychloroquine has shown major success when used early in high-risk people but, as one would expect for an antiviral, much less success when used late in the disease course.
- Delays in waiting before starting the medications can reduce their efficacy.
- FDA concerns about the drug did not announce is that these adverse events were generated from tens of millions of patient uses of hydroxychloroquine for long periods of time, often for the chronic treatment of lupus or rheumatoid arthritis.
- The harms are minuscule compared to the mortality occurring right now in inadequately treated high-risk COVID-19 patients.
https://web.archive.org/web/20200723155027/https://www.newsweek.com/key-defeating-covid-19-already-exists-we-need-start-using-it-opinion-1519535
- As of May 27, 2020 there are over 1,678,843 confirmed cases of COVID-19 claiming more than 100,000 lives in the Unites States. Currently there is no known effective therapy or vaccine.
- •According to a protocol-based treatment algorithm, among hospitalized patients, use of hydroxychloroquine alone and in combination with azithromycin was associated with a significant reduction in-hospital mortality compared to not receiving hydroxychloroquine.
- •Findings of this observational study provide crucial data on experience with hydroxychloroquine therapy, providing necessary interim guidance for COVID-19 therapeutic practice.
https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext
Dr. Harvey Risch, an epidemiology professor at Yale School of Public Health, said on Tuesday that he thinks hydroxychloroquine could save 75,000 to 100,000 lives if the drug is widely used to treat coronavirus.
“There are many doctors that I’ve gotten hostile remarks about saying that all the evidence is bad for it and, in fact, that is not true at all,” Risch told “Ingraham Angle,” adding that he believes the drug can be used as a “prophylactic” for front-line workers, as other countries like India have done.
Risch lamented that a “propaganda war” is being waged against the use of the drug for political purposes, not based on “medical facts.”
Researchers at the Henry Ford Health System in Southeast Michigan have found that early administration of hydroxychloroquine makes hospitalized patients substantially less likely to die.
https://www.foxnews.com/media/hydroxychloroquine-could-save-lives-ingraham-yale-professor
JRC Publishing LLC, New Jersey has published an important book on treatment of COVID-19 virus. The book is based on medical research and treatment conducted by Dr. Roland Derwand, Prof. Martin Scholz and Dr. Zelenko.
The compendium presents treatment process and detailed experiences of COVID-19 patients while undergoing medical care with Dr. Zelenko and his colleagues from around the world. This extensive work, covering 248 pages, offers unparalleled breath of medical research and is the first volume to be published in this field to date. The e-book is available for download and is being distributed free of charge.
https://internetprotocol.co/covid-19/2020/07/21/yale-harvard-professors-support-zelenkos-protocol/
The Recovery trial has steadfastly ignored Professor Didier Raoult and a string of countries that have implemented his protocol, early use of HCQ with Azythromycin in safe doses, despite the fact that, after treating 3,737 patients — the single largest study in the world —Raoult has lost only 0.6 per cent, while Horby and Landray are presiding over carnage —a fatality rate of 25 per cent.
- The Recovery trial has steadfastly ignored Professor Didier Raoult in the early use of HCQ with Azythromycin in safe doses.
- Raoult has lost only 0.6 per cent, while Horby and Landray are presiding over carnage —a fatality rate of 25 per cent.
- Landray admitted to an investigative journalist at FranceSoir ‘these are quite high doses to… have a chance of killing the virus.’ Or killing the patient.
- Recovery is not the only trial delivering dangerously elevated doses of HCQ to Covid patients. Dosage in the international Solidarity trial was four times greater than the dose being used in India.
- WHO has been working for years with Gilead Sciences trying to get the pharmaceutical company’s lacklustre drug Remdesivir to show efficacy at curing first Ebola, with poor results, and now Covid-19.
- Landray revealed Gilead pays scientists 20 to 50 times more to conduct a clinical trial than Horby and Landray were paid to conduct the Recovery trial.
- Horby is the executive director of the International Severe Acute Respiratory and Emerging Infection Consortium which received 4.5 million pounds for research into vaccines.
- Horby established the Epidemic Research Group which is promised up to 14 million pounds from AstraZeneca and Zuckerberg/Chan of Facebook fame for the development of a Covid-19 vaccine which is being trialled by Oxford University.
- AstraZeneca is interested in merging with Gilead Sciences, which, if it went through, would create the biggest Big Pharma ever.
- Horby and Landray have announced that dexamethasone, a low-cost steroid which is also being tested has reduced the mortality rate of Covid-19 patients on ventilators from a scandalous 41 per cent to a still appalling 32 per cent.
- Raoult has pointed out that in his hospital, of the 0.6 per cent who die, a mere 16 per cent were in ICU
- In Britain, where almost 42,000 people have died of Covid, the only thing randomised, controlled trials have achieved, is to blind people to the evidence that 40,000 of those deaths could have been avoided.
https://www.spectator.com.au/2020/06/bring-on-britains-corona-clowns/p>
- Non-COVID patients were put in with COVID patients, then marked with Do Not Resuscitate orders.
- Hospitals have a financial incentive to mark patients as COVID-19.
- Doctors stopped treating people as humans. Inexperienced doctors were practicing on patients.
- COVID-19 has been proven to be easily treatable with the Hydroxychloroquine/Zinc/Antibiotic protocol
- People were coming in too late due to fear.
- Patients were unnecessarily put on ventilators. “They want to use the vents.”
- Patients were put in restraints “due to laziness.”
- New York may have been hit hard because their hospitals were already struggling. They couldn’t afford to keep them open.
More than 1.6 million Americans have been infected with SARS-CoV-2 and >10 times that number carry antibodies to it. High-risk patients presenting with progressing symptomatic disease have only hospitalization treatment with its high mortality. An outpatient treatment that prevents hospitalization is desperately needed. Two candidate medications have been widely discussed: remdesivir, and hydroxychloroquine+azithromycin. Remdesivir has shown mild effectiveness in hospitalized inpatients, but no trials have been registered in outpatients. Hydroxychloroquine+azithromycin has been widely misrepresented in both clinical reports and public media, and outpatient trials results are not expected until September. Early outpatient illness is very different than later hospitalized florid disease and the treatments differ. Evidence about use of hydroxychloroquine alone, or of hydroxychloroquine+azithromycin in inpatients, is irrelevant concerning efficacy of the pair in early high-risk outpatient disease. Five studies, including two controlled clinical trials, have demonstrated significant major outpatient treatment efficacy. Hydroxychloroquine+azithromycin has been used as standard-of-care in more than 300,000 older adults with multicomorbidities, with estimated proportion diagnosed with cardiac arrhythmias attributable to the medications 47/100,000 users, of which estimated mortality is <20%, 9/100,000 users, compared to the 10,000 Americans now dying each week. These medications need to be widely available and promoted immediately for physicians to prescribe.
https://academic.oup.com/aje/advance-article/doi/10.1093/aje/kwaa093/5847586