High COVID-19 vaccination rates were expected to reduce transmission of SARS-CoV-2 in populations by reducing the number of possible sources for transmission and thereby to reduce the burden of COVID-19 disease. Recent data, however, indicate that the epidemiological relevance of COVID-19 vaccinated individuals is increasing. In the UK it was described that secondary attack rates among household contacts exposed to fully vaccinated index cases was similar to household contacts exposed to unvaccinated index cases (25% for vaccinated vs 23% for unvaccinated). 12 of 31 infections in fully vaccinated household contacts (39%) arose from fully vaccinated epidemiologically linked index cases. Peak viral load did not differ by vaccination status or variant type.
Viral Load
Browse the articles related to this topic below.
Join our community on Guilded.
High COVID-19 vaccination rates were expected to reduce transmission of SARS-CoV-2 in populations by reducing the number of possible sources for transmission and thereby to reduce the burden of COVID-19 disease. Recent data, however, indicate that the epidemiological relevance of COVID-19 vaccinated individuals is increasing.
…The US Centres for Disease Control and Prevention (CDC) identifies four of the top five counties with the highest percentage of fully vaccinated population (99.9–84.3%) as “high” transmission counties.
Public health officials and the medical establishment with the help of the politicized media are misleading the public with assertions that the COVID-19 shots provide greater protection than natural immunity. CDC Director Rochelle Walensky, for example, was deceptive in her October 2020 published LANCET statement that “there is no evidence for lasting protective immunity to SARS-CoV-2 following natural infection” and that “the consequence of waning immunity would present a risk to vulnerable populations for the indefinite future.”
Peter McCullough, MD, MPH speaks at the 78th Annual Meeting of AAPS on October 2, 2021.
Presentation notes:
- 1min: Something was going very wrong very early in 2019.
- 2m: The threshold for shutting down a new biologic product is just a few cases.
- 3m: Covid-19 was going to be the showcase of what we could do for biotech.
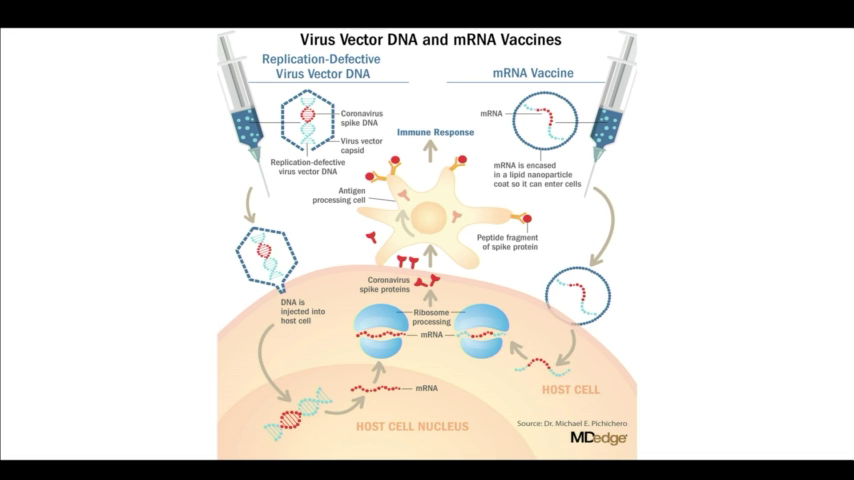
- 5m: The spike protein created by the new Covid-19 is a deadly protein.
- 11m: Our institutions are all culpable in medical malfeasance.
- 13m: We have the biggest biological catastrophe on our hands with a medicinal product in human history…and no-one knows how to stop it.
- List of risk
- 14m: 86% of deaths have no other explanation other than the vaccines.
- 20m: We are in freefall into a lawless state. The Vaccines are not safe for use on either side of the Atlantic. It’s clear that this first generation of [Covid-19] vaccines is not safe.
- 22m: The FDA did not approve Pfizer. The gave a continuation of the emergency use authorization and then conditionally approved Comirnaty with BioNTech which is legally and potentially medicinally distinct. The Pfizer approval is a false talking point.
- 23m: When Pfizer came up for boosters, McCullough and his team presented at the FDA showing that death with the vaccine is greater than death just taking your chances with the infection. The vaccines aren’t safe across the board and the panel agreed 16:2 against the booster.
- 26m: Data for the efficacy of the vaccines do not take into account the Delta variant. These vaccines have failed against Delta and other variants. Two-thirds who get sick with Delta are fully vaccinated. Data shows that the vaccines can’t stop transmission.
- 27m: Effectiveness for Pfizer is at 42%. A vaccine that falls below 50% protection and can’t last a year is not a viable product. Pfizer has failed as a commercial product.
- 29m: The CDC was telling us in May 2021 that the vaccines were failing. They started to do asymmetric reporting to craft a narrative that this was going to be a crisis of the unvaccinated but the CDC data showed the opposite. The ineptitude and willful misconduct of the people running our public health agencies is astounding.
- 32m: The ‘99% of hospitalized were unvaccinated’ message was a propagandized false talking point because the data is not there.
- 33m: The vaccines have had zero impact on the epidemic curve. Mortality is a function of treatment.
- 34m: Many experts have been warning that we shouldn’t vaccinate into a pandemic because it creates resistance. As soon as we started vaccinating, the number of strains starting falling. The virus was figuring out how to thrive in the vaccinated.
- 36m: The Delta variant has achieved antigenic escape. The data shows that the vaccinated is an equal threat to the unvaccinated.
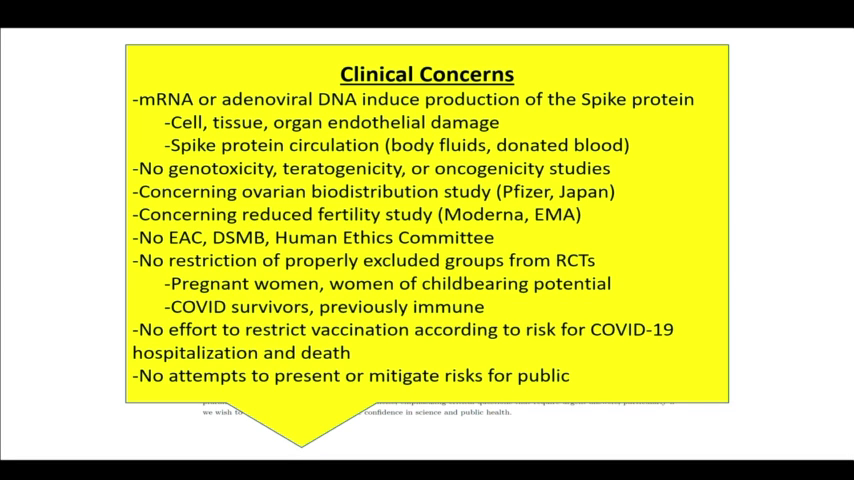
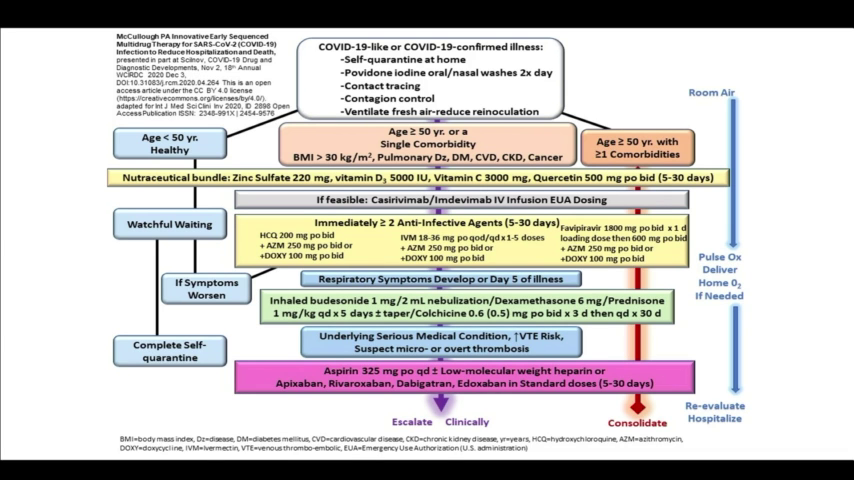
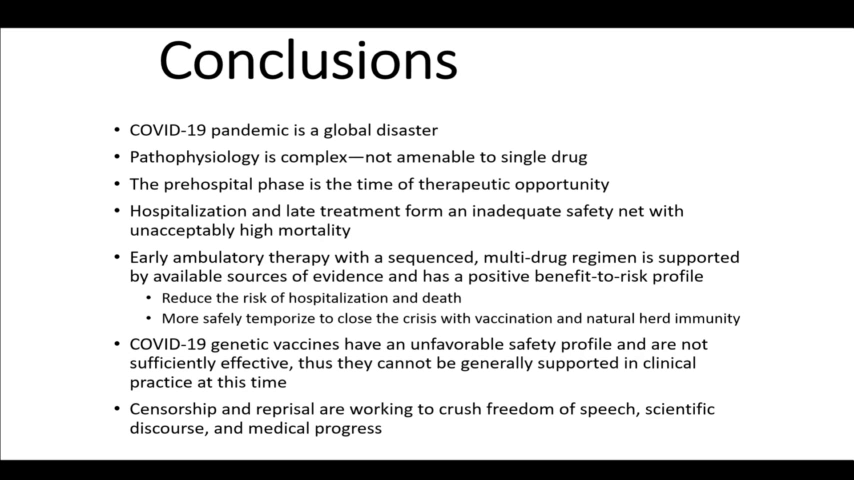
- 38m: Early home treatment is the only thing that makes sense. That’s what it should have always been.
- 40m: Doctors at my institution cannot look me in the eye because they are so ashamed of what they’ve done during the course of this pandemic.
- 44m: If you look through the clinical records [of those who have died] and I will tell you they were all inadequately treated.
- 50m: Natural immunity is superior to vaccine immunity. If we vaccinate people who are covid-recovered, we harm them considerably. The only backstop is natural immunity.
File download:
A Guide to Home-Based COVID Treatment from the Association of American Physicians and Surgeons – PDF (1.4MiB)
Slides:
Backup mirrors:
Dr. Philip McMillan interviews vaccine developer Geert Vanden Bossche and Robert Malone MD, inventor of mRNA vaccine platform.
Interview highlights
- Geert Vanden Bossche (GV) at 17m: Massive surges of the infection rates, especially in countries with an aggressive mass-vaccination policy, was predictable.
- Robert Malone (RM) at 23m: The Israeli data is a concern: we are seeing signs that the durability of the [Pfizer vaccine] is very poor.
- RM at 26m: The vaccinated are a higher risk of becoming superspreaders because they’re replicating virus at the same or higher levels than the unvaccinated but they feel better.
- GV at 28m: The effect of mass-vaccination is an ideal breeding-ground for more infections spread. However, if still have a substantial proportion that is non-vaccinated, you will see a reduction of infectious pressure.
- GV at 31m: The unvaccinated are ‘the vaccum cleaners’ who will eliminate a lot of virus from the population by mounting long-lived immunity and contribute to the reduction of infectious pressure. The vaccinated cannot contribute to the infectious pressure.
- RM at 33m: The truth is that it’s the vaccinated that are creating the risk, not the unvaccinated. The unvaccinated are serving as virus sinks. The probability of them having significant disease and death is minute. The real risk is the vaccinated who have received very focused spike proteins.
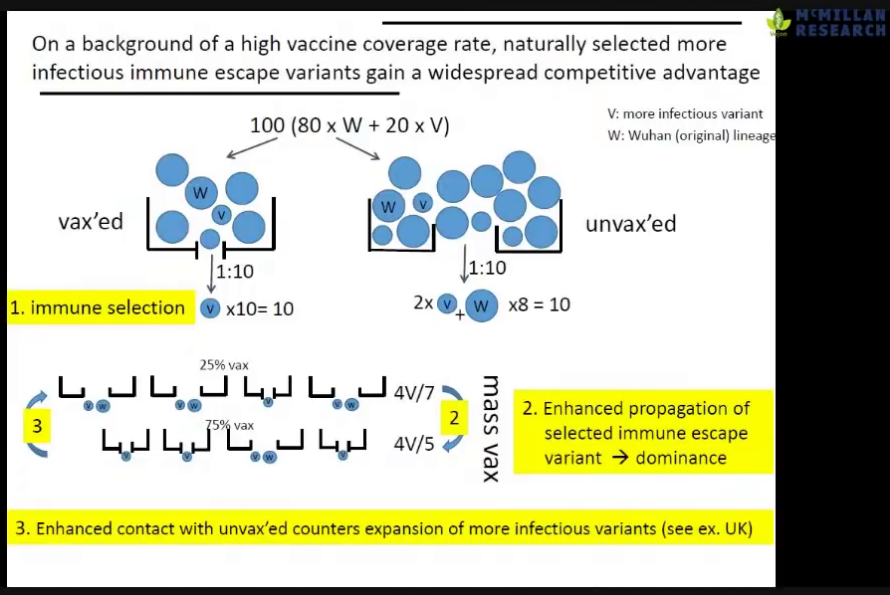
- GV at 35m: It is not a problem of individuals being vaccinated. The problem is a policy of mass-vaccination. That is how the more infections variant can adapt to the population and become dominant.
- GV at 58m: Young people are now getting the disease pretty fast because of the increased infectious pressure [due to mass-vaccination].
- RM at 1h10m: There are disincentives to asking questions about data for vaccine-enhanced replication and antibody-dependent enhancement; no-one wants fund the studies.
- GV at 1h12m: Regulators have no experience with the current situation where there are very many unknowns when deploying a new vaccine to the public.
- RM at 1h17m: The FDA is not structured to detect adverse advents and have admitted they cannot evaluate safety. Two of the top [US] regulators resigned because the FDA is no longer independent from the policy-making apparatus which exists in the Executive Branch [of US Government].
- RM at 1h24m: There is an intrinsic conflict of interest in the CDC in that it is funded to promote vaccines but also has the under-funded mission of evaluating their safety.
- RM at 1h25m: Policy recommendations together with Peter Navarro (American economist and author):
- Reserve vaccines for the high-risk population and make it available globally.
- Make early interventions [like Ivermectin and Vitamin D] widely available. Many are very effective when administered early and aggressively.
- Make home-test kits available (acknowledging that they have a bias to false positives) and make more specific tests in physicians offices.
- Address the fear by showing that currently most people are not at risk.
- GV at 1h30m: The most important thing is to reduce the infectious pressure. This is a huge threat to all those who were naturally protected, such as young people. The worst thing to do is to vaccinate the younger age groups because they are ‘the buffer’ of long-lived immunity. They are our hope for herd immunity. We will not get herd immunity from mass-vaccination.
- GV at 1h39m: We need to compare the ratio of severe disease of deaths in vaccinated and unvaccinated. We are seeing more case fatalities in the vaccinated but the numbers are not being made available.
- RM at 1h41m: There is a persistent signal in the UK data that there seems to be an excess deaths in the vaccinated and yet a relative deficit in the vaccinated. This is paradoxical.
- GV at 1h47m: Discrimination against the non-vaccinated is complete scientific nonsense. We should care about susceptibility. What is relevant is how can we protect ourselves best.
Slides:

Backup mirrors:
The public is being threatened by the government…It doesn’t leave much room in their direction of travel…Look to Austrailia

This means that whilst vaccination may reduce an individual’s overall risk of becoming infected, once they are infected there is limited difference in viral load (and Ct values) between those who are vaccinated and unvaccinated. Given they have similar Ct values, this suggests limited difference in infectiousness.
In yet another unexpected and unwelcome twist in the pandemic, the Centers for Disease Control and Prevention released on Friday a report strongly suggesting that fully immunized people with so-called breakthrough infections of the Delta variant can spread the virus to others just as readily as unvaccinated people.
The concern that SARS-CoV-2 could be spread by people without symptoms originally came from a single case report. It was alleged that an asymptomatic woman from China had spread the virus to 16 other contacts in Germany. Later reports showed that, at the time of contact, this woman was taking medication for flu-like symptoms, invalidating the evidence provided for the theory of asymptomatic transmission. As with other common respiratory viruses, SARS-CoV-2 spreads by being exhaled, coughed or sneezed into the air. The largest droplets fall quickly and settle on the ground whilst the most lightweight particles, known as aerosols, may remain suspended in the air for days. Once the virus is present in the environment, it spreads by finding its way into the respiratory tract of new hosts in a large enough quantity (known as the ‘viral load’ or ‘infectious dose’) to infect them. The theory of fomite transmission (touching contaminated surfaces and then touching the face) is not supported by scientific evidence.
…In asymptomatic individuals, the viral load is typically very low and the infectious period is also short in duration. They may still exhale virus particles, which another person may encounter. However, the overall likelihood of transmitting the disease to others is negligible. Thus asymptomatic cases are not the major drivers of epidemics. As Dr Anthony Fauci of the US National Institute of Allergy and Infectious Diseases stated in March 2020: ‘In all the history of respiratory-borne viruses of any type, asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is always a symptomatic person.’
Conclusions: The majority of studies report identification of SARS-CoV-2 RNA on inanimate surfaces; however, there is a lack of evidence demonstrating the recovery of viable virus. Lack of positive viral cultures suggests that the risk of transmission of SARS-CoV-2 through fomites is low. Heterogeneity in study designs and methodology prevents comparisons of findings across studies. Standardized guidelines for conducting and reporting research on fomite transmission is warranted.
“We have to stop the nonsense. We have entered a vicious cycle. With every new wave, we’re starting a new wave of lockdowns. The lockdowns are creating a new virus. Then we have a new epidemic. We’re starting a new lockdown that creates a new virus.”
Transcript
To guard against censorship, a transcript from https://dryburgh.com has been archived below. Please visit the source in the following link: https://dryburgh.com/knut-wittkowski-lockdowns-are-creating-a-new-virus/
Dr Knut Wittkowski
Dr. Wittkowski received his PhD in computer science from the University of Stuttgart and his ScD in Medical Biometry from the Eberhard Karls University of Tübingen, both Germany. He worked for 15 years with Klaus Dietz, a leading epidemiologist who coined the term “reproduction number”, on the Epidemiology of HIV before. Around 1990, he was one of the few to predict that HIV would not spread among Caucasian heterosexuals. After teaching epidemiology at the University of Cairo and the American University of Beirut, he was for 20 years head of Biostatistics, Epidemiology, and Research Design at The Rockefeller University, New York.
Dr. Wittkowski is currently the CEO of ASDERA LLC, a company discovering novel interventions against complex diseases from data of genome-wide association studies, including a nutritional intervention to reduce cellular support for virus replication and to improve cardiovascular and metabolic health as a natural strategy to reduce the burden and stop the continuation of the COVID epidemics.
Updates
- March 23rd, AP News: Chancellor of Germany Angela Merkel “We basically have a new pandemic. Essentially we have a new virus, obviously of the same type but with completely different characteristics. Significantly more deadly, significantly more infectious, and infectious for longer.” (Germany extends virus lockdown till mid-April as cases rise)
Transcript
Host ➝ 00:00
Welcome. Today it’s for anyone who may or may not know me, I am Tania The Herbalist, and today I have the privilege of talking and chatting with Knut Wittkowski. Knut is not any medical expert, actually. He’s got a master’s in biostatistics, a PhD in computer science, a doctor of science and medical biometry, including genetics and epidemiology. And you were former head of research, design and biostatistics at the Rockefeller Foundation.
Knut Wittkowski ➝ 00:36
And epidemiology at the Rockefeller University here in New York.
Host ➝ 00:42
Beautiful. Thank you for that. Well, you now have gone viral because of your expertise and your many articles and especially one of your most recent ones about how much lockdown policy does not actually agree with the established epidemiological policy. Because, of course, we know the experts controlling the local policy are motivated by fear and politics. Can you talk about that a little bit for us?
Knut Wittkowski ➝ 01:12
If we go back one year and if you still remember the reason for having a lockdown, people were afraid that the situation in the US, and in particular in New York, at the time would become as dire as in the North of Italy where the hospital system was totally overwhelmed.
And one could understand that even though I didn’t share that fear, but I could understand it. But a month later we had the data from the CDC that there would never be a major problem.
The hospital ship that had anchored in New York left. The Javits center, the conference center that had 2000 beds, was never used. The tents in Central Park put up by Mount Sinai hospital, also not used.
There was a shortage here and there, once in a while, but there was no, not even close to the hospital system collapsing.
So one could have reopened and said, well, it was three, four weeks, too bad. We were overly pessimistic, overly careful, but everybody would have understood that was erring on the side of caution.
Knut Wittkowski ➝ 02:52
And then suddenly the game posts shifted. It was not anymore about the hospital system collapsing. Today it’s not either.
We have currently something like less than 15% of all hospital utilization is due to COVID. That is noticeable, but it doesn’t mean that there is a major problem.
Again, there may be a local problem here or there, but that is not, should not be enough to run the whole economy against the wall.
So it became somewhat unclear what the objective of the lockdown should be. Should it be that the country should be locked down until there is no single virus around anymore? Somehow nobody actually explained that. Why should we control the virus? Why should we stop the spread? And could we?
Host ➝ 04:11
Right. So, from your expertise, what is the difference between COVID and influenza?
Knut Wittkowski ➝ 04:22
If we had not the tools to sequence the virus and had learned in late December [2019] or early January [2020], I forgot when it was, that this happened to be a coronavirus, one of those that hit us every now and then, rather than influenza virus that hits us a bit more frequently, we would not have seen any difference between this and the epidemic, for instance, of 2017/2018, which was also a bad flu.
Host ➝ 04:59
Right. And now if we let it run its course the way we do other viruses, how long do you think it would actually be before we could reach herd immunity?
Knut Wittkowski ➝ 05:08
It will take about six weeks and can be shifted a bit in different parts of the country, depending on where the virus gets there [“endemic equilibrium herd immunity”].
So it was here in New York earlier, and the epidemic ended even before the lockdowns started. I mean, that infections went down before the lockdown started. It came later in the South.
So in the South, we have seen the effect of flattening the curve. You are delaying the infections and illnesses and death for a couple of months until you reopen. And then the delayed events happen because lockdowns do not prevent anything from happening. They just delay it a bit.
Host ➝ 05:59
Is there any scientific background behind lockdowns?
Knut Wittkowski ➝ 06:04
Nobody has ever done a lockdown for any disease. So it was not quite clear how this experiment would end.
Host ➝ 06:16
Right, right. And so many are actually are, sorry, go ahead.
Knut Wittkowski ➝ 06:22
And what we saw was that it backfired in many ways. So one thing that we have seen, and we know since October, when the viruses in Spain and France had been sequenced, we know that because of the lockdowns giving the virus enough time to mutate, we had escape mutations that started the wave in November. So we are currently experiencing the result of the lockdowns. Without lockdowns, we would not have any COVID right now.
Host ➝ 07:06
Right. And it’s funny because many seem to argue that the lockdown measures is actually what decreased the potential mortalities that could have happened if it wasn’t for these measures. So really, how effective are the measures like social distancing, isolation, things like that.
Knut Wittkowski ➝ 07:22
They’re very effective. They have cost many jobs and the economy a lot of money. So they were very effective [sarcasm].
Host ➝ 07:32
Right, right. And here in Ontario, I’m in Canada in Ontario here, we’ve now got a stay at home order. So, you know, even things like going to bargaining and skating and things like that outdoors, they’re almost saying, don’t do, stay at home. Only leave for essentials
Knut Wittkowski ➝ 07:51
Because otherwise, we need that [restrictions breeding variants] urgently, because otherwise we run the risk that there will be no new epidemic in a few months [sarcasm]. Because the lockdowns are essential for the virus to develop new strains.
“because of the lockdowns giving the virus enough time to mutate, we had escape mutations that started the wave in November. So we are currently experiencing the result of the lockdowns. Without lockdowns, we would not have any COVID right now.”
Our immune system develops typically something like five or six different types of antibodies to protect us from mutations that might happen while we are infected to make sure that even if there is a mutation in one of the epitopes, the targets of the antibodies, if there is a mutation, then there should be other antibodies that still are sufficient to prevent the virus from being replicated and from spreading.
However, if you give the long enough and the virus mutates at a rate of one or two mutations a month. So if you give it three months, there’s a good chance that there will be six consecutive mutations, one for each of these antibodies.
And at the end, the human immunity does not capture the virus anymore. And the virus can spread.
We have, even though it’s technically mostly the same virus, but experience as if it were a totally new virus. And this is what we’re seeing right now.
“Nobody has ever done a lockdown for any disease. So it was not quite clear how this experiment would end.”
What we have seen since November is a new virus, or actually a family of new viruses, because similar things happened in Spain and France and in the UK and in South Africa and also in the United States. So it’s a very… the common thing, if you give the virus enough time with the lockdowns, it will mutate and you have the next epidemic.
Host ➝ 09:51
Right. And how important is it for us to be outdoors and being with nature and being outside and getting fresh air? Because I think a stay at home orders, I believe could be obviously detrimental, especially for the healthy and the young and children.
Knut Wittkowski ➝ 10:07
I mean, I don’t want to go there. It’s too frustrating to see a whole generation of children being deprived of their wellbeing and their development.
The children can not, it’s immunologically dramatic, because they cannot develop the immune responses that they need for the rest of their life.
They don’t have the social contacts that they have in school. They don’t learn.
If you’re taking away one year in the development – and it’s now getting more than that – one year in the development of a child that’s below the age of 10, you’re creating a huge gap and you’re preventing this child from having all the opportunities that they otherwise would have. And the tragic thing here is that there is no reason for it.
Children do not get ill – with very rare exceptions.
Yes, we have had in the United States, something like – I haven’t checked the last week.
So maybe it’s 30 deaths in children from age four to age fourteen. Thirty. We had over 50 from influenza during the same time period. Yes. It happens with every flu, a few children die. And I feel sorry for the families who are affected. For them, it’s a tragedy.
However, should we close down the country of 335 million people in the US, a bit less in Canada, but should we destroy the life of hundreds of millions of people, because there is a risk for some children. And most of these children who die have co-morbidities, have diabetes, have other diseases, other immune diseases. The balance, this is totally out of balance.
Host ➝ 12:51
Yeah. And at what point in time did you realize that these measures are going to kill more people than prevent?
Knut Wittkowski ➝ 13:01
That was known from the very beginning because the measures do not reduce COVID deaths, but they’re causing lots of others.
And so we knew from the very beginning that there would be more deaths because of the lockdowns, unless we are counting the risk that the hospital system would collapse and then we would have many deaths for other reasons.
But as soon as it was clear that the hospital system would not be collapsing – and it still is not collapsing – the lockdowns should have ended.
And the schools should never have been closed, because children, except for the very rare exceptions, don’t develop any severe illness. So they will not end up in a hospital.
Even the young adults don’t end up in hospitals in relevant numbers. We knew that 50% of all people who died, many of them in hospitals, were older than 80 years.
So if you are below the age of 60, your risk of having a severe disease or even dying is irrelevant. I mean, when we cross the street, we can always be hit by a brick and still not everybody wears hard hat all the time, because there is a theoretical risk that you may be hit by a brick.
And here, for those under the age of 60, about, it is a theoretical risk, like the many theoretical risks that we are facing every day in our life.
“That was known from the very beginning because the measures do not reduce COVID deaths, but they’re causing lots of others.”
And we have to take risks because otherwise we couldn’t live. And that’s what we have right now. We cannot live.
Host ➝ 15:17
Now. I have to ask you, how is the data for COVID being collected now in comparison to previous respiratory infections?
Knut Wittkowski ➝ 15:29
I have been working many years ago on HIV when I predicted correctly that HIV would never spread among the Caucasian heterosexual population, which at that time, politicians and media were very scared of. They thought all of Europe and the United States would become depopulated because of HIV. Didn’t happen.
But there actually, the reporting was good. We knew for every case and then “case” meant you have the disease, you have a problem. So for every case, it was reported, when was it diagnosed, and when was it reported.
So these days, the difference were there. And as epidemiologists, we could use that to make more sense of the data and the definitions were not changed all the time [unlike with COVID-19].
I just learned today that it seems that PCR, the definition of what a positive PCR test is, is being changed from running for 35 cycles to only running for 25 cycles, which makes the test less sensitive.
And then of course, we know that the vaccines are working [sarcasm] because there are fewer infections, except at the same time, the test was changed.
And we had had so many changes. What is a “case”? A case traditionally is somebody who has an illness, and then you find out why that person is ill.
Right now you have people who want to travel or have a job requirement. So they’re standing here on the street to get tested. And if they happened to get tested positive, they are called a case. They’re not ill, they probably will never be. They may not even be infected. They may just have some virus sitting in the nose that never got into the body. And you call them cases? Everything in this epidemic is done upside down. It almost feels like people want to obscure what’s going on because we know that during an epidemic, you don’t change the measures that you take, because then you cannot compare it anymore. And here it happens all the time, which is frustrating.
Host ➝ 18:28
Now I have to ask you because of course I admire your courage and you speaking out against this, but why do you find that more medical experts are not speaking about this, especially when you hear about MDs and even some neurologists, but you’re never hearing about a virologist or an epidemiologist that are really speaking out on this, which, like yourself, are the best people.
Knut Wittkowski ➝ 18:50
We have three virologists speaking out in the United States and only virologists. Different areas of science have different objectives. And people are trained for doing different things.
“Everything in this epidemic is done upside down. It almost feels like people want to obscure what’s going on”
An MD is trained to make a diagnosis with an individual patient, find the treatment, convince the patient that he or she should take the treatment, follow up and see how it works. This is by and large, what an MD is treated to do.
A virologist studies the structure of the virus. What is it composed of and where does it bind? And how does the cell with the virus binds, interact with the cell? How can, what would be potential vaccine? How, what structure, what epitopes would we use? Things like that.
And then there are epidemiologists who study how does the virus spread? What is the most effective thing to do against the spread of the virus? These questions, no MD and no virologist is trained to deal with these questions because you need mathematical models. You need a lot of experience in dealing with large sets of data, and that is something what epidemiologists do, and they were not heard in March or April.
Host ➝ 20:40
Now, one of the last questions that I have to ask you, of course, just to kind of give people a little bit of light because many are starting wake up more and more about the lockdowns kind of being worse than the disease itself, because there’s a lot of implications. What do you think is the proper solution to handle this virus? If you had the option, what’s your solution.
Knut Wittkowski ➝ 20:59
Okay. The first thing you already said, let’s reopen schools and the economy. There’s no reason to keep them closed.
Of course, masks can be helpful when worn by those who are vulnerable, and let’s presume masks are effective, and we’re still not quite sure whether they are, but let’s presume that they’re effective. And this would be one of the strategies, the vulnerable, those who have comorbidities and are older can use to pre-protect themselves, to self isolate while the virus is running among the low risk people and taking its natural course, which will have very few severe events and very few deaths. Because as I said, it is mostly the elderly who die.
So masks should be worn by those who are vulnerable and by the people who directly interact with the vulnerable, because if you are helping somebody from the wheelchair into the beds, or the other way around there is physical interactions and close proximity. And these are situations where the risk of transmission is highest. And so to help the elderly or the vulnerable to self isolate, those directly interacting with them should wear a mask.
And also, if possible, try to distance a bit. Everybody else should not because if everybody else does the same thing, then the vulnerable wouldn’t have an advantage anymore. The virus would spread a bit more slowly overall. It would spread at the same rate among the elderly and vulnerable as among the young and healthy.
So if everybody wears a mask and does other ways of distancing, we are increasing the number of deaths.
So just to put the numbers that we have in context. In the United States, we had so far about 400,000 deaths, 200,000 were from COVID-20, since November, which would not have been here without lockdowns.
Knut Wittkowski ➝ 23:42
And then among those among 200,000, 40% were in nursing homes. Now the nursing homes – we’ve been talking about protecting the vulnerable. If the vulnerable had been protected better, there would have been much fewer deaths. There may have been about a hundred thousand. A hundred thousand deaths is normal for a flu. It’s at the upper end, but this is nothing unusual for flu.
So we should keep everything open and we should focus on the things that are really dangerous. It’s not dangerous to be coughing or sneezing for a few days while you have a flu or even COVID like many people have.
It gets dangerous when you end up in the hospital, in the emergency room and then you may die. So we have to prevent that. And now I’m talking a bit pro domo. My company is working on something like that. One of these strategies where we are giving people the option to prevent, to reduce their comorbidities.
And without comorbidities, almost nobody dies.
Knut Wittkowski ➝ 25:16
And also to reduce the rate by which the virus spreads in the body, within the body. Because we are not dying of the virus itself. We could live with that virus forever. It would produce a couple of viruses on the side, but that’s not a big deal.
“There may have been about a hundred thousand. A hundred thousand deaths is normal for a flu. It’s at the upper end, but this is nothing unusual for flu.”
What we are dying off is the immune system. When it has the antibodies. After one week of incubation time, the immune system kills all infected cells. And if many cells are infected, like in the lung, then a large part of the lung cells are being killed. Now that’s causing a problem. If people are young and healthy, they can live with it. If they’re old and a bit fragile, that huge wound is killing them. So it’s the reaction of the immune system to the virus that’s killing. And that depends, how dangerous it is, depends on the viral load.
Knut Wittkowski ➝ 26:26
So when we can reduce the rate by which the virus replicates it’s by only 10%, then for every seven hour replication cycle. Then after the five days, we have reduced the number of cells that became infected by about 80 to 90%. And then the wound created by the immune system is much smaller and everybody survives it.
So we should not close down schools and the economy, we should focus on helping the elderly and vulnerable to self isolate. And we should also focus on dealing with the one problem that is really important, and that is preparing the immune system better to deal with that infection in a natural way so that the disease is not so severe. And if the disease is not so severe, then what are we talking about?
We are not closing the country down for the common cold. And if we succeed in reducing the severity of that disease to that of a common cold, and I think that is possible. And even if it were to the severity of a regular flu, then why do we need to lock down?
Host ➝ 28:07
All right. Thank you for that information, Knut. Is there anything else that you would want to add to any of this?
Knut Wittkowski ➝ 28:20
I think we covered most of the things. The advice to our politicians is very simple. I am not the only one. If you think of the Great Barrington Declaration that has been signed now by over a million scientists.
Knut Wittkowski ➝ 28:45
We have to stop the nonsense. We have entered a vicious cycle. With every new wave, we’re starting a new wave of lockdowns. The lockdowns are creating a new virus. Then we have a new epidemic. We’re starting a new lockdown that creates a new virus.
Einstein defined the word insanity, and said, insanity is doing the same thing over and over again, and expecting different results. Doing lockdowns over and over again will have no other results than creating the viruses that are capable of starting a new epidemic. And then we are exactly at the point where we were before.
Although it may be a bit worse because the new virus may also be resistant against some of the cross immunity that we already had from other coronavirus infections. So we may need more people to get infected, to get over the next virus.
Knut Wittkowski ➝ 30:13
And then I have one fear.
And that is that every new generation of viruses here, the virus genome gets closer and closer to the human genome because our immune system can make antibodies only against stretches of genetic information on the genome that are unique to the virus.
And just a couple of weeks ago, three weeks or so, a paper was published and there it said less than 10% of the virus genome is available for the immune system to make antibodies against it. And then every generation, the virus mutates and becomes a bit closer to something that is already in the human genome. And then it becomes more and more difficult for the immune system to make antibodies. This situation has never arrised in the whole history of humankind. The lockdowns are creating a problem that has never existed. And for which nature did not find a solution. We should let nature do it. We should adjust. We should adapt. But we should not think that we can control nature.
Knut Wittkowski ➝ 32:06
My first name is Knut, and I had a namesake in the 11th century, more or less exactly a thousand years ago. And he got annoyed by people thinking he was so powerful he could do anything.
And so he walked to the beach and told the tide to stay away. Just to show that nature was much more powerful than even the most powerful King at the time. Of course the tide didn’t stay away.
“With every new wave, we’re starting a new wave of lockdowns. The lockdowns are creating a new virus. Then we have a new epidemic.”
Now, since then, during the last 1000 years, I don’t think there was a single politician who would have said nature is more powerful than I am. Politicians think they know everything better, everything better than nature. And they can control a virus like the tide. We cannot control the tide and we can not control a virus. We can only make it worse.
Host ➝ 33:25
Very well said, very well said. It’s true. Let nature run its course is really the ultimate thing that we can do for proper herd immunity and getting back to some form of normalcy. So I appreciate your wisdom. I appreciate your words. And I appreciate your work, Knut. Where can people find you if they want to connect with you on your website? I don’t know if you’re on social media, where can they connect with you more?
Knut Wittkowski ➝ 33:51
My name is unique. If you look for Knut Wittkowski, you will find me.
“We have to stop the nonsense. We have entered a vicious cycle. With every new wave, we’re starting a new wave of lockdowns. The lockdowns are creating a new virus. Then we have a new epidemic. We’re starting a new lockdown that creates a new virus.”
Host ➝ 34:00
Right. And, of course, your website is asdera.com. You’ve got lots of information there. So anyone who’s looking for it, interviews, articles, everything that you’ve done.
Knut Wittkowski ➝ 34:18
I will put this there too, as soon as it gets published. So thank you, Tania.
Host ➝ 34:25
Well, thank you so much for your time. Thank you. I appreciate it. And we’ll do this again hopefully soon sometime. Thank you.
Conclusions and Relevance In this cohort study, there was no evidence of placental infection or definitive vertical transmission of SARS-CoV-2. Transplacental transfer of anti-SARS-CoV-2 antibodies was inefficient. Lack of viremia and reduced coexpression and colocalization of placental angiotensin-converting enzyme 2 and transmembrane serine protease 2 may serve as protective mechanisms against vertical transmission.
WHO has received user feedback on an elevated risk for false SARS-CoV-2 results when testing specimens using RT-PCR reagents on open systems.
As with any diagnostic procedure, the positive and negative predictive values for the product in a given testing population are important to note. As the positivity rate for SARS-CoV-2 decreases, the positive predictive value also decreases. This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as positivity rate decreases, irrespective of the assay specificity. Therefore, healthcare providers are encouraged to take into consideration testing results along with clinical signs and symptoms, confirmed status of any contacts, etc.