Dr. John Campbell seems surprised at the Office for National Statistics Freedom of Information request about deaths from COVID-19 with no other underlying causes.
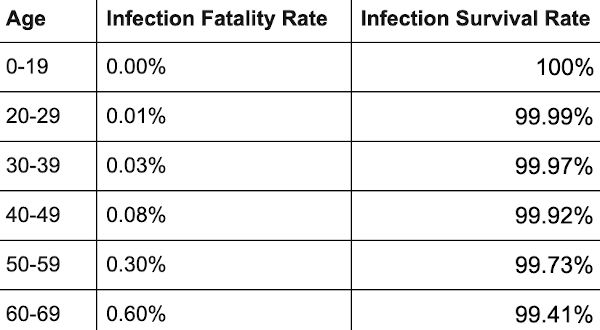
Age Groups
Browse the articles related to this topic below.
Join our community on Guilded.
Commentary from Paul Embery of UnHerd:
Fresh NHS data shows that the total number of covid-related deaths in hospitals in England involving patients under the age of 80 and with no pre-existing condition is 3,037. This covers the entire period of the pandemic.

Dr. Peter A. McCullough, MD, MPH, is a board-certified cardiologist who has testified before committees of the US and Texas Senate regarding the treatment of COVID-19 and management of the ongoing pandemic.
Backup mirrors:
However, despite this apparent evidence to support vaccine effectiveness – at least for the older age groups – on closer inspection of this data, this conclusion is cast into doubt. That is because we have shown a range of fundamental inconsistencies and flaws in the data. Specifically:
• In each group the non-Covid mortality rates in the three different categories of vaccinated people fluctuate in a wild, but consistent way, far removed from the expected historical mortality rates.
• Whereas the non-Covid mortality rate for unvaccinated should be consistent with historical mortality rates (and if, anything slightly lower than the vaccinated non-Covid mortality rate) it is not only higher than the vaccinated mortality rate, but it is far higher than the historical mortality rate.
• In previous years each of the 60-69, 70-79 and 80+ groups have mortality peaks at the same time during the year (including 2020 when all suffered the April Covid peak at the same time). Yet in 2021 each age group has non-Covid mortality peaks for the unvaccinated at a different time, namely the time that vaccination rollout programmes for those cohorts reach a peak.
• The peaks in the Covid mortality data for the unvaccinated are inconsistent with the actual Covid wave.
Whatever the explanations for the observed data, it is clear that it is both unreliable and misleading. We considered the socio-demographic and behavioural differences between vaccinated and unvaccinated that have been proposed as possible explanations for the data anomalies, but found no evidence supports any of these explanations. By Occam’s razor we believe the most likely explanations are:
• Systematic miscategorisation of deaths between the different groups of unvaccinated and vaccinated.
• Delayed or non-reporting of vaccinations.
• Systematic underestimation of the proportion of unvaccinated.
• Incorrect population selection for Covid deaths.
On Thursday, the government published its 44th vaccine surveillance report and in a table on page 18 it noted 2,032 deaths of double-vaccinated individuals over 70. More than 3,000 from the same double-jabbed cohort were hospitalised.
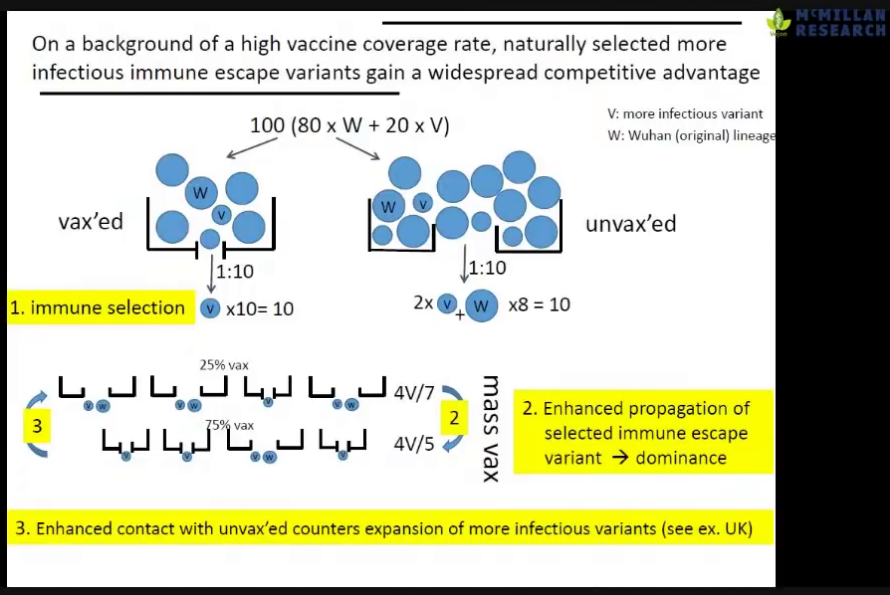
Dr. Philip McMillan interviews vaccine developer Geert Vanden Bossche and Robert Malone MD, inventor of mRNA vaccine platform.
Interview highlights
- Geert Vanden Bossche (GV) at 17m: Massive surges of the infection rates, especially in countries with an aggressive mass-vaccination policy, was predictable.
- Robert Malone (RM) at 23m: The Israeli data is a concern: we are seeing signs that the durability of the [Pfizer vaccine] is very poor.
- RM at 26m: The vaccinated are a higher risk of becoming superspreaders because they’re replicating virus at the same or higher levels than the unvaccinated but they feel better.
- GV at 28m: The effect of mass-vaccination is an ideal breeding-ground for more infections spread. However, if still have a substantial proportion that is non-vaccinated, you will see a reduction of infectious pressure.
- GV at 31m: The unvaccinated are ‘the vaccum cleaners’ who will eliminate a lot of virus from the population by mounting long-lived immunity and contribute to the reduction of infectious pressure. The vaccinated cannot contribute to the infectious pressure.
- RM at 33m: The truth is that it’s the vaccinated that are creating the risk, not the unvaccinated. The unvaccinated are serving as virus sinks. The probability of them having significant disease and death is minute. The real risk is the vaccinated who have received very focused spike proteins.
- GV at 35m: It is not a problem of individuals being vaccinated. The problem is a policy of mass-vaccination. That is how the more infections variant can adapt to the population and become dominant.
- GV at 58m: Young people are now getting the disease pretty fast because of the increased infectious pressure [due to mass-vaccination].
- RM at 1h10m: There are disincentives to asking questions about data for vaccine-enhanced replication and antibody-dependent enhancement; no-one wants fund the studies.
- GV at 1h12m: Regulators have no experience with the current situation where there are very many unknowns when deploying a new vaccine to the public.
- RM at 1h17m: The FDA is not structured to detect adverse advents and have admitted they cannot evaluate safety. Two of the top [US] regulators resigned because the FDA is no longer independent from the policy-making apparatus which exists in the Executive Branch [of US Government].
- RM at 1h24m: There is an intrinsic conflict of interest in the CDC in that it is funded to promote vaccines but also has the under-funded mission of evaluating their safety.
- RM at 1h25m: Policy recommendations together with Peter Navarro (American economist and author):
- Reserve vaccines for the high-risk population and make it available globally.
- Make early interventions [like Ivermectin and Vitamin D] widely available. Many are very effective when administered early and aggressively.
- Make home-test kits available (acknowledging that they have a bias to false positives) and make more specific tests in physicians offices.
- Address the fear by showing that currently most people are not at risk.
- GV at 1h30m: The most important thing is to reduce the infectious pressure. This is a huge threat to all those who were naturally protected, such as young people. The worst thing to do is to vaccinate the younger age groups because they are ‘the buffer’ of long-lived immunity. They are our hope for herd immunity. We will not get herd immunity from mass-vaccination.
- GV at 1h39m: We need to compare the ratio of severe disease of deaths in vaccinated and unvaccinated. We are seeing more case fatalities in the vaccinated but the numbers are not being made available.
- RM at 1h41m: There is a persistent signal in the UK data that there seems to be an excess deaths in the vaccinated and yet a relative deficit in the vaccinated. This is paradoxical.
- GV at 1h47m: Discrimination against the non-vaccinated is complete scientific nonsense. We should care about susceptibility. What is relevant is how can we protect ourselves best.
Slides:

Backup mirrors:
Categories
The elephants in the room – PANDA
While citizens focus on the latest issue the government directs our attention to, many of us have lost sight of the big picture and grown accustomed to severe limitations on our rights like the proverbial frogs in hot water. As a number of countries now seek to focus the discussion on further coercive measures and even mandatory vaccination, PANDA is increasingly aware of the elephants in the room, the topics no one is talking about.
http://archive.today/2021.09.16-104523/https://www.pandata.org/elephants-in-the-room/
Teenage boys are six times more likely to suffer from heart problems from the vaccine than be hospitalised from Covid-19, a major study has found.
Children who face the highest risk of a “cardiac adverse event” are boys aged between 12 and 15 following two doses of a vaccine, according to new research from the US.
We write as concerned doctors, nurses, and other allied healthcare professionals with no vested interest in doing so. To the contrary, we face personal risk in relation to our employment for doing so and / or the risk of being personally “smeared” by those who inevitably will not like us speaking out.
The by now all-too-familiar vertiginous lines were intended to leave the public in no doubt about the consequences of not delaying freedom until July 19.
But take a closer look and the choice of graphs is arguably disingenuous: the slides are most revealing for what they failed to include.

https://www.telegraph.co.uk/news/2021/06/15/fear-freedom-doom-laded-government-graphs-dont-show-us/
Dr. Peter McCullough has been the world’s most prominent and vocal advocate for early outpatient treatment of SARS-CoV-2 (COVID-19) infection in order to prevent hospitalization and death. On May 19, 2021, I interviewed him about his efforts as a treating physician and researcher. From his unique vantage point, he has observed and documented a profoundly disturbing policy response to the pandemic—a policy response that may prove to be the greatest malpractice and malfeasance in the history of medicine and public health.”
Link to interview audio format released by Julian Charles of The Mind Renewed podcast.
Backup mirror:
I had no choice but to speak out against lockdowns. As a public-health scientist with decades of experience working on infectious-disease outbreaks, I couldn’t stay silent. Not when basic principles of public health are thrown out of the window. Not when the working class is thrown under the bus. Not when lockdown opponents were thrown to the wolves. There was never a scientific consensus for lockdowns. That balloon had to be popped.
…Ultimately, lockdowns protected young low-risk professionals working from home – journalists, lawyers, scientists, and bankers – on the backs of children, the working class and the poor.
https://www.spiked-online.com/2021/06/04/why-i-spoke-out-against-lockdowns/
Levels of antibodies in the blood of vaccinated people that are able to recognise and fight the new SARS-CoV-2 Delta variant first discovered in India (B.1.617.2) are on average lower than those against previously circulating variants in the UK, according to new laboratory data from the Francis Crick Institute and the National Institute for Health Research (NIHR) UCLH Biomedical Research Centre, published today (Thursday) as a Research letter in The Lancet.
The results also show that levels of these antibodies are lower with increasing age and that levels decline over time, providing additional evidence in support of plans to deliver a vaccination boost to vulnerable people in the Autumn.
In the case of single-dose recipients, our data show that NAbTs are significantly lower against B.1.617.2 and B.1.351 VOCs relative to B.1.1.7, implying that although a single dose might still afford considerably more protection than no vaccination, single-dose recipients are likely to be less protected against these SARS-CoV-2 variants. These data therefore suggest that the benefits of delaying the second dose, in terms of wider population coverage and increased individual NAbTs after the second dose,7 must now be weighed against decreased efficacy in the short-term, in the context of the spread of B.1.617.2. Worldwide, our data highlight the ongoing need to increase vaccine supply to allow all countries to extend second-dose protection as quickly as possible.
In the longer term, we note that both increased age and time since the second dose of BNT162b2 significantly correlate with decreased NAb activity against B.1.617.2 and B.1.351—both of which are also characteristic of the population in the UK at highest risk of severe COVID-19 (ie, older and vaccinated earlier), independent of other existing factors such as compromised immune status or comorbidity, or geographic-specific responses to vaccination.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)01290-3/fulltext
All under-40s are to be offered an alternative to the Oxford-AstraZeneca coronavirus vaccine as a precaution.
Dr. Sucharit Bhakdi, a Thai-German microbiologist, discusses mRNA vaccines, blood clots and Cerebral Venous Thrombosis. He warned about the vaccine side-effects months before the roll-out and appears to have been proven correct.
Rob Verkerk, Founder, Executive and Scientific Director of the Alliance for Natural Health International, a scientist who has for 30 years been exploring positive ways to span the gulfs between science and the law, between academia and industry, and between governments and their people.
Backup mirror:
Johnson & Johnson (J&J) has expanded Phase IIa clinical trial of Covid-19 vaccine candidate to include adolescent subjects aged 12 to 17 years.
https://www.clinicaltrialsarena.com/news/johnson-vaccine-trial-adolescents/
“Those errors are when introducing people of more than one hundred years, it has happened that they are figurative as that those deceased have 1 year, or 2, or 3 instead of 101, 102 or 103 “, considers one of them,” Pere Soler, pediatrician of the Infectious Pathology and Pediatric Immunodeficiencies unit of the Vall d’Hebron hospital explains.
One year on from the start of the first lockdown, the brutal price of this drastic policy is all too obvious. Amid battered public finances, rising unemployment and widespread business failures, entire sectors of the economy have been devastated.
…Indeed, the average age of Covid fatalities is over 82, higher than the UK’s average age of death from all causes. And among those who contract the disease, just two in 1,000 (or fewer) actually die.
…But, while every death is a tragedy for bereaved families, 7 per cent above average does not strike me as a particularly shocking figure, especially since some of those deaths were caused by lockdowns themselves.
…In fact, there is no authoritative research that reveals a clear correlation between the severity of lockdowns and the avoidance of viral peaks.