2:55 – Masks
• Tom Jefferson: “Aside from people who are exposed on the frontlines, there is no evidence that masks make any difference, but what’s even more extraordinary is the uncertainty: we don’t know if these things make any difference…. We should have done randomised control trials in February, March and April but not anymore because viral circulation is low and we will need huge number of enrolees to show whether there was any difference”.
• Carl Heneghan: “By all means people can wear masks but they can’t say it’s an evidence-based decision… there is a real separation between an evidence-based decision and the opaque term that ‘we are being led by the science’, which isn’t the evidence”.
9:26 – Pandemic life cycle
• CH: “One of the keys of the infection is to look at who’s been infected, which shows a crucial difference when comparing the pandemic theory to seasonal theory. In a pandemic you’d expect to see young people disproportionately affected, but in the UK we’ve only had six child deaths, which is far less than we’d normally see in a pandemic. The high number of deaths with over-75s fits with the seasonal theory”.
14:00 – Covid seasonality
• CH: “The stability of the virus is far less when the temperature goes up but humidity seems to be particularly important. The lower the humidity, the more stable the virus is in the atmosphere and on surfaces… It’s now winter in the southern hemisphere, which is why places like Australia are suddenly having outbreaks.”
20:37 – Lockdown
• CH: “Many people said that we should have locked down earlier, but 50% of care homes developed outbreaks during the lockdown period so there are issues within the transmission of this virus that are not clear… Lockdown is a blunt tool and there needs to be intelligent conversations about what mitigation strategies can keep society functioning while we keep the most vulnerable shielded”.
25:20 – Nightingale hospitals
• CH: “They are the wrong structure. What you need is fever hospitals which were here until around the 1980s or 90s. They were on single floors and had isolation within isolation. Theere were no lift shafts and staff were trained, which meant that everyone was protected from each other… It looks like at leats 20% of people got the infection while they were in hospital”
27:30 – Suppression strategy
• CH: “The benefits of the current strategy are outweighed by the harms…When it comes to suppression, only the virus will have a determination in that. If you follow the New Zealand policy of suppressing it to zero and locking down the country forever, then you’re going to have a problem… This virus is so out there now, I cannot see a strategy that makes suppression the viable option. The strategy right now should be how we learn to live with this virus”
32:45 – Response to the virus
• TJ: “I am a survivor of four pandemics and for the other three, I didn’t even realise they were going on. People died but nothing changed and none of the fabric of society was eroded like this response… Do I see steps being taken at a European level about learning from our mistakes and changing policies? The answer is no…
39:30 – Politics of the virus
• CH: “We as individuals are part of the problem because sensationalism drives people to click and read the information. So it’s a big circle because we’ve created the problem — if we put the worst case scenario out there, we will go and have a look. If you want a solution, you’ve got to get people to stop clicking on this sensationalist stuff”.
43:30 – IFR
• CH: “We will be down about where we were with the swine flu: around 0.1-0.3% which is much lower than what we think because at the moment we are seeing the case fatality”.
• TJ: “If you look at the whole narrative, it was distorted from the very beginning by the obsession with influenza which was just one or two agents and nothing else existed. We’re no different now”.
Videos
An archive of videos and podcasts with a link to the original source or backup mirror.
Browse the articles related to this topic below.
Join our community on Guilded.
Key quotes:
• There was “massive confusion” about different Covid data between England’s health bodies. “Public Health England figures are about double the ONS figures because PHE are reporting anybody who has had a positive Covid death in the past… This will get increasingly confusing as we go into the next Winter because there could be a new outbreak and new deaths while also still reporting on historical deaths… This is a problem for epidemiologists and media… ”
• Even a “28 period cut-off is still not ideal for accurate death numbers because there is “immediate cause and underlying cause… Immediate cause means you’ve had Covid within 21 days but outside of that, it becomes the underlying cause — something that contributed to your death but wasn’t a direct cause. A 21 day cut-off would be helpful because it gives a clearer understanding of that distinction”
• “We follow excess deaths which is the most accurate information about what’s going on at that moment, but it can’t tell you what those deaths are caused by” (i.e. people not coming forward with heart attacks etc)
• “There’s an important distinction between lives lost and life years lost. One of the things we’ll be watching very closely over the next six months is how many people would have actually died in the next six months… That’s where the excess deaths really matter. If we start to see it trend significantly under for the next few months, we’ll start to come forward with information that suggests there was a group of vulnerable people that any respiratory infection would have shortened their life.”
• “In the media you’ll always hear about catastrophe and the consequences of that. One of the things we notice is that when you don’t hear anything that usually means there’s good news happening. So when Sweden looks worse you hear about it but when it’s not so bad, like now, you never see it in the media.”
References for the video can be found at the content creator’s website at https://the-iceberg.net
Screenshot of article from News West 9 that has been taken down:

“Intensive care units are getting empty, the wards are getting empty, we are really seeing a decrease — and that despite that people are really loosening up. The beaches are crowded, social distancing is not kept very well … but still the numbers are really decreasing. That means that something else is happening – we are actually getting closer to herd immunity. I can’t really see another reason.”
“I can’t say if the Swedish approach was right or wrong – I think we can say that in one or two years when we are looking back. You have to look at the mortality over the whole period.”
“I don’t think that we have more new cases, I think we are just detecting more cases”
“We found that if you have a mild case you can be negative for antibodies afterwards … in those almost all of them had strong T-cell activity. This study says that there are cases that you can have a strong T-cell response even though you have not had antibodies, meaning that you have encountered the virus and built up immunity.”
Interview highlights:
- We have already developed herd immunity to COVID-19 and will continue to manage it through herd immunity.
- Flu is much more dangerous than COVID-19.
- COVID-19 will settle into an endemic state just like flu.
- Hopefully vaccines will be important in protecting the vulnerable.
- Another way to protect the vulnerable sector is to allow the population to develop natural immunity.
- There’s no reason to think the virus will mutate into a lower level of virulence.
- During the 1918 flu because of a large number of ‘immunologically naive’ individuals but this is not the case with COVID-19.
- Most of us have some degree of coronavirus immunity and therefore some protection to COVID-19.
- The current H1 influenza strain is antigenically identical to the 1918 flu. H1 flu doesn’t kill as many people as the 1918 flu because most people already have cross immunity.
Mirror:
Laura Dodsworth interviews Alistair Haimes on Freethinking with Laura Dodsworth.
Support Laura Dodsworth through Patreon:
https://www.patreon.com/lauradodsworth
Interview notes and charts
- The difference between what the government was telling us and what their information was telling us was so extreme and outrageous.
- Exponential means a “constant rate of growth.” The government data in March was clearly showing that the COVID-19 was declining, not growing exponentially. This was the same in all countries you could see the data. [See chart 1]
- A constantly declining growth rate will make a bell curve. The government were standing in front of bell curve graphs during their briefings yet they were telling us we were in the middle of the epidemic.
- It was very clear that we were heading to a peak sometime around early to mid-April.
- You don’t have to be complicated mathematics to see that COVID-19 was running out of steam almost from day one.
- The conclusion from the Centre for Evidence-Based Medicine seems to be that it’s impossible to predict if there will be a second wave.
- Sweden’s epidemic looks identical to the UK’s but they did not lockdown. Their datapoint indicates there won’t be a second wave. There has been no spike in Denmark either. [See chart 2]
- Unknowns: has summer affected COVID-19 and will there be a mutation?
- Will illnesses during the autumn and winter be mis-attributed to COVID-19? Poor media coverage means that we can’t be sure.
- Symptoms of COVID-19 are very similar to the flu. Something could look like a second wave but will we really know?
- The lockdown is costing a Brexit bill a week.
- The government response seems to have been skewed by Neil Ferguson’s modelling data. The make-up of government advisors seems to be a recipe for groupthink, which is very dangerous.
- Epidemiology (the way a disease spreads through the population) is not complicated science. The government could have had lots of people who were very good at this but they didn’t.
- We should have cocooned the vulnerable, make sure the NHS has capacity and “let it rip” through the population.
- We should never have had an open-ended lockdown.
- The ‘R number’ is just the difference of in the number of people infected after each generation of a disease. Britain crossed the ‘magical R of 1’ line a few days before lockdown and the same day as Sweden. Whatever interventions have been done doesn’t seem to have had any effect. [See chart 3]
- COVID-19 is mostly a care home and hospital disease. This was obvious very early on. Old people should not have been moved from hospitals into care homes. It seems as if we knowingly seeded the most vulnerable environment with the disease.
- 37% of our deaths are care home residents but they are only 0.5% of our population. Of them are dementia sufferers.
- Over 20% of the infections were picked up in the hospitals. COVID-19 seems more like MRSA than influenza in that it’s an infection control problem.
- COVID-19 is much more comparable to flu for the rest of the population.
- 1968 flu killed 80,000 people in the UK.
- This last winter was a low flu winter. It’s quite possible that the people who died of COVID-19 are those who didn’t die.
- If you overlay COVID-19 deaths with the 2000 flu season, they look very similar. [See chart 4]
- 95% of deaths have had another serious disease. Most people have almost no chance of dying from COVID-19.
- If you are under 40, you have more chance of being struck by lightning that dying of COVID-19.
- If you are under 60, you have more chance of drowning.
- At any age, you have more chance of dying on the roads than dying of COVID-19.
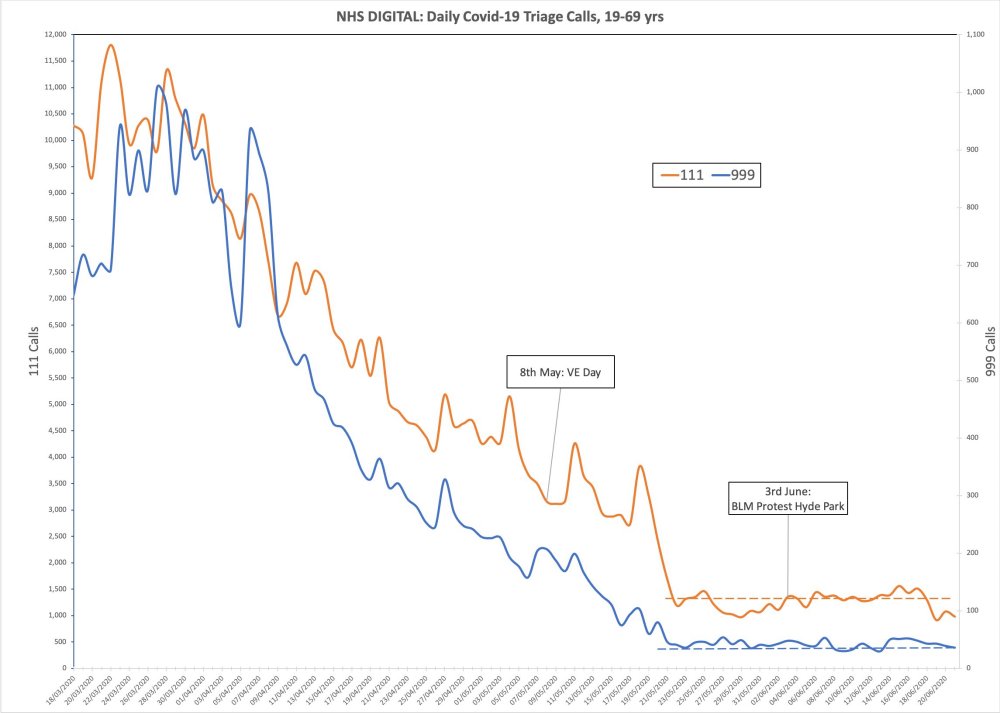
- Lead indicators of 111 and 999 calls with COVID-19 symptoms show there was no spike after VE Day celebrations or BLM protests. In fact, it was even coming down at lockdown. That lockdown was big change for COVID-19 is invisible in the data. [See chart 5]
Charts
Chart 1: COVID-19 was declining in Europe as of march. It was not growing exponentially
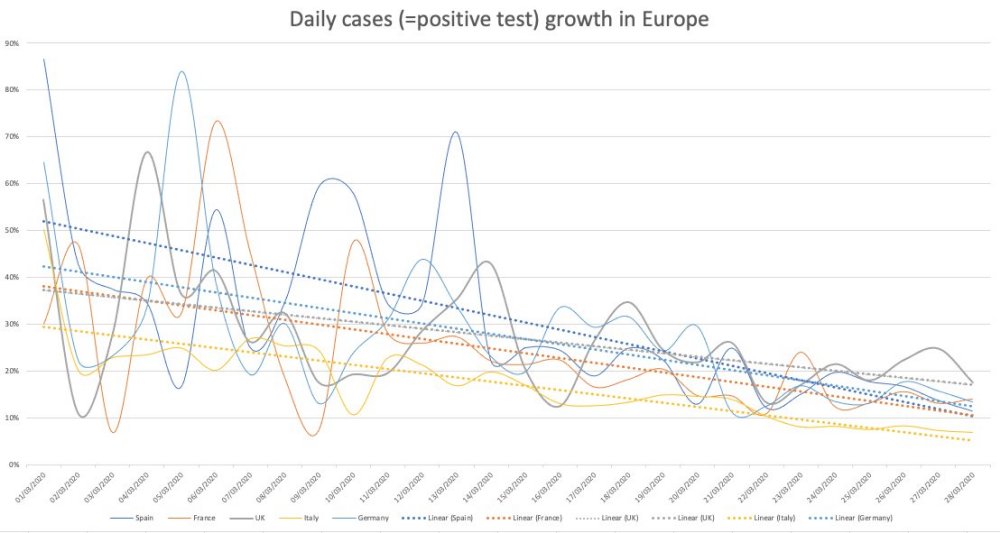
Chart 2: Sweden’s epidemic looks similar to the UK’s but they did not lock down.
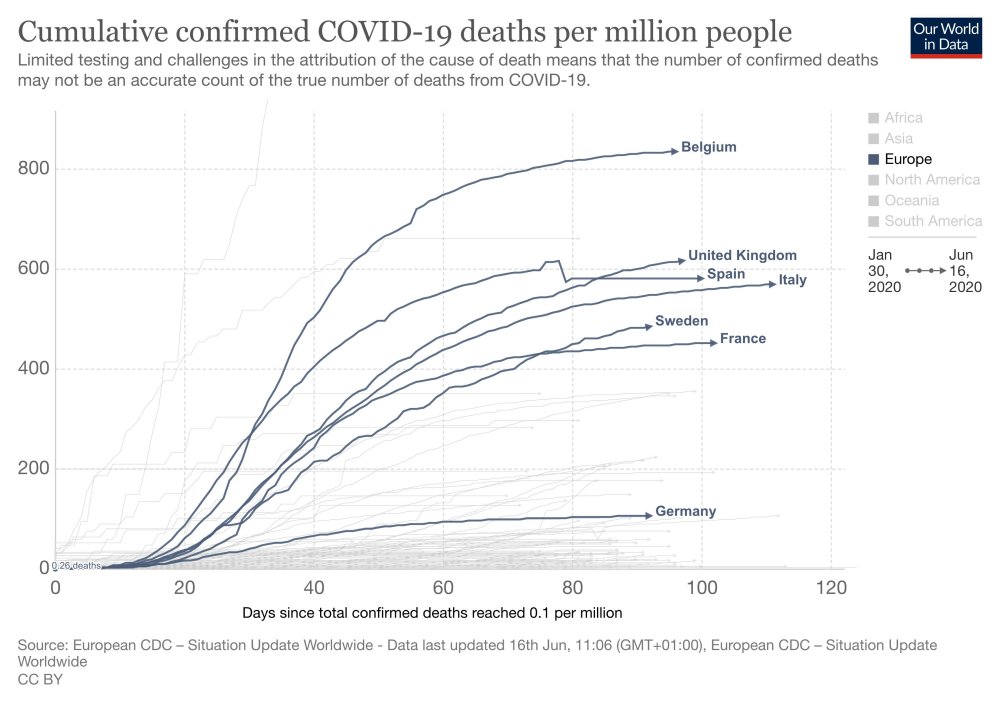
Chart 3: Britain crossed the ‘magical R of 1’ line a few days before lockdown

Chart 4: COVID-19 deaths overlayed with the 2000 flu season
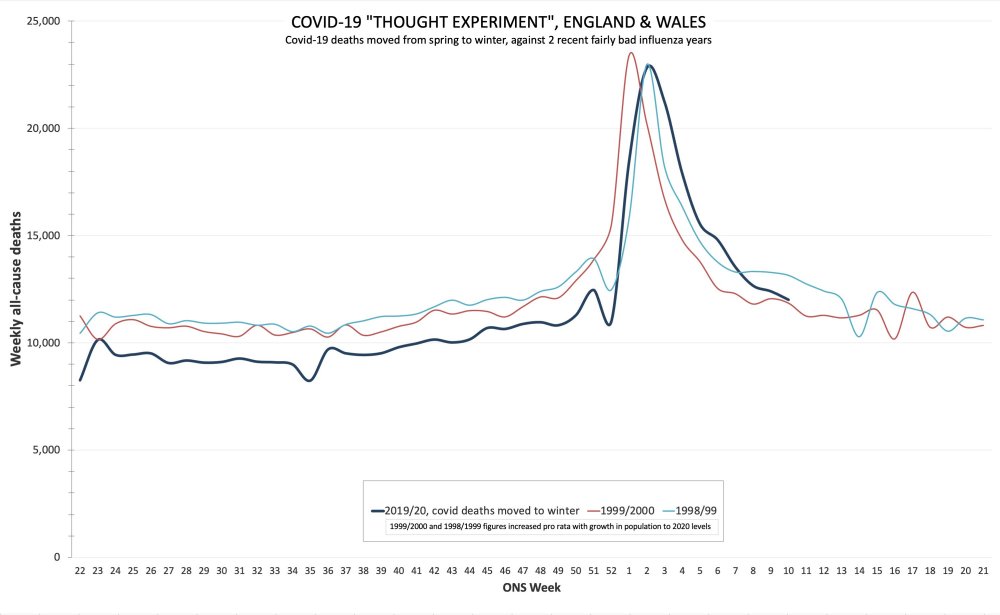
Chart 5: No spike after BLM protests
- Non-COVID patients were put in with COVID patients, then marked with Do Not Resuscitate orders.
- Hospitals have a financial incentive to mark patients as COVID-19.
- Doctors stopped treating people as humans. Inexperienced doctors were practicing on patients.
- COVID-19 has been proven to be easily treatable with the Hydroxychloroquine/Zinc/Antibiotic protocol
- People were coming in too late due to fear.
- Patients were unnecessarily put on ventilators. “They want to use the vents.”
- Patients were put in restraints “due to laziness.”
- New York may have been hit hard because their hospitals were already struggling. They couldn’t afford to keep them open.
Maria Van Kerkhove, head of the World Health Organization’s emerging diseases and zoonosis unit, says transmission of the coronavirus by people who aren’t showing symptoms is “very rare.” She spoke Monday at a briefing in Geneva.
Mirrored video:
Note: The video has been removed from Vimeo but has been archived on BitChute (see embedded below highlights).
James talks with Professor Dolores Cahill, a world renowned immunologist who has advised the Irish government and the EU.
- We should end the lockdown. Quarantining healthy people was a huge mistake, should never have been done and should never happen again.
- All the available information tells us there’s no longer any basis for the lockdowns. The economic harm and resulting health effects could be five times higher than those caused by the virus. The adverse health implications of poverty is well-known and has lots of supporting data.
- The immunology community knew in January and February that there was nothing very special about COVID-19.
- There are lots of clinical trials showing the usefulness of vitamins C, D and Zinc for preventing symptoms of corona-type viruses.
- It is also very well established that hydroxychloroquine, which is a very safe drug, can be used as a treatment.
- There was no need to ramp up the hospital care system because there were established methods for prevention and treatment.
- It was known that the virus would circulate the world in a month. Professor Cahill was surprised at the lockdown because the ‘virus was gone.’ There is clearly enough data for this.
- COVID-19 (also known as SARS-CoV-2) is about 80% the same as SARS-CoV-1 in 2003. These types of viruses last about 6 weeks in each location before naturally ‘dying off’ as people become exposed and then developing immunity.
- 80 out of 100 people would have developed antibodies within 10-11 days and become immune for life without experiencing symptoms.
- Although COVID-19 is a novel virus, it can be ‘recognized’ by the immune system of anyone who had already been exposed to SARS-CoV-1. This is because of COVID-19’s 80% similarity to the earlier 2003 virus.
- With these types of viruses, you will be negative for the PCR test (which tests for the presence of the virus) after recovery but you will test positive for the antibodies.
- You don’t need the lockdown if you boost your immune system. in fact, the lockdown made matters worse by depressing people’s immune system. Sunshine, interacting with people, shaking hands–all these help to boost your immune system.
- Elderly people should be taking vitamin C, D and Zinc to protect their immune systems. People with underlying conditions, or those who develop symptoms, should contact their doctor to consider prescribing off-label hydroxychloroquine.
- Symptoms: flu-like for the first five days. If it gets worse and you develop a cough, that’s when you need to ring your doctor for treatment. Treatment includes hydroxychloroquine for 3-5 days, with Zinc and AZT antibiotic. This is an established protocol that has been used in many clinical trials in 2020.
- There was some reason to be scared of COVID-19 during the very early stages (around January) because because we didn’t know anything about it. However, the media and WHO was fearmongering when they used Wuhan as an example of what would happen everywhere.
- From February onward, the immunology community recognized that COVID-19 is the same as a normal virus in most parts of the world. There was something different about Wuhan, Bergamo and New York but t here was no reason to lockdown the rest of the world.
- Vaccines have their place and can be safe. However, studies show that animal and human subjects that were given a type of influenza vaccine later reacted badly when they encountered a coronavirus ‘in the wild’. The reaction caused a cytokine storm that either killed the subject or made the subject very ill. The reaction between different types of vaccinated and wild viruses is called viral interference.
- People in Wuhan and Bergamo were given a certain type of influenza vaccine. It became apparent around April-May that the high death rates in both cities could be due to viral interference from the administered influenza vaccine.
- It has not been possible to make a safe and effective vaccine for the SARS-CoV-1 in 2003. If we have not been able to make a vaccine for this coronavirus, we should not expect a safe vaccine for COVID-19 any time soon. A vaccine developed for COVID-19 would be a complete experiment on those who take it.
- Vaccines containing alluminium, Thimerodal or mercury are intrinsically unsafe.
- The global death rate for COVID-19 is around the same as a bad influenza. Outside of Wuhan, Bergamo and New York, the death rate appears to be less than the normal flu.
- Current data shows that the real death rate for COVID-19 is 20 or 30 times less than the initial estimates from the WHO. We now know the death rate is about one in a thousand for the vulnerable and one in five thousand for the healthy. In the under 70s age range, this is lower than the average flu.
- It was well-known in February that there was no need for the lockdowns.
- There have been no cases of transmission from children.
- If we were to end the lockdown, we would need 10 days to prepare. This is because people have not been out and exposed to sunlight. Preparation include taking vitamins C, D and Zinc; getting fresh air; avoiding stress; and making sure doctors have hydroxychloroquine.
- It is almost as if the current advice is geared to making sure people get sick in order to support more lockdowns.
- There will be no second spike if people take the above precautions to strengthen their immune system.
- A recent study shows that people who continued working were healthy. Engaging with other keeps you healthy by strengthening the immune system.
- There hasn’t been an open debate in any country about the harm versus benefits of the lockdown. This may be a big reason for why the lockdowns are continuing.
- Dr. Rashid A. Buttar and Dr. Judy Mikovits are trying to open the debate about prevention and treatments but their voices are being censored.
- The use of hydroxychloroquine as a treatment has been politicized.
- Evidence is being cherry-picked in order reach a predetermined goal: a money-making vaccine. The existing prevention and treatment methods don’t make money for big-pharma.
- Masks and social distancing is appropriate for something like ebola but not for coronaviruses.
- We will build up herd immunity within about two weeks.
- We know how COVID-19 is transmitted because it belongs to the family of coronaviruses. It is not transmitted through the air. This has been proven because groups of people in encloses spaces (for example, plane-loads of fruit-pickers) did not all come down with the sickness.
- The two meter rule is unnecessary.
- There was enough information from many sources for the government and their advisors to know that all these measures are wrong. There should be legal implications for those who advocate continued lockdown. Hundreds of unnecessary deaths should be grounds for a legal tribunal.
- There is a high risk of a death spike after lockdown due to other causes, such as cancers, that will attributed to COVID-19. This will be used to support more lockdowns.
- The politicians, broadcasters, newspaper editors, ministers for health–everyone complicit in censoring and withholding information from the public about the true nature of COVID-19 needs to be held personally liable for the deaths caused.
- There was genuine fear at the beginning but the COVID-19 response is now political.
- Nothing at the beginning of the epidemic justified the subsequent reaction.
- The community suffered from ascertainment bias: hospitals saw the worst form of the virus so they thought we were dealing with a big problem.
- Lockdown means people will be getting nastier versions of the virus.
- We implemented a policy of enormous magnitude without considering the implications. This goes against the most fundamental principle of medicine.
- A significant number of the excess deaths are not victims of COVID-19 but of the lockdown. More than half of the deaths may be found due to other causes.
- The response of the authorities and media has made it impossible to understand what was going on.
- Our huge and emotional overreaction has caused more harm.
- Years of life lost is a more important metric than the number of deaths.
- Most people working in the NHS wouldn’t speak out about these things.
- There were two types of journalism during the epidemic: investigative journalism and illustrative journalism (propaganda). Most of the mainstream media were engaged in propaganda and ended up frightening the people and the government. They need to take their share of the responsibility of the damage caused.
- COVID-19 is nowhere near as bad as previous epidemics.
- The medical establishment should have been speaking out since the beginning of the lockdown. The evidence was pretty clear, pretty quickly.
- Vaccine is a red herring because it’s unlikely we’re going to have one. The Common Cold Research Institute spent 43 years trying to make a vaccine for the common cold and didn’t manage it.
- Track and Trace is extremely worrying and not thought-through with its implications for a Big Brother society. None of it makes sense.
- Social distancing is nonsense. Vulnerable people should be given information and allowed to make their own decisions.
- The NHS is there to protect us. That’s what we pay our taxes for.
- Young people are being thrown in the scrapheap for a disease that isn’t going to affect them.
- As you get older, your immune system starts to ‘forget’ diseases you’ve already had. That’s why older people are more susceptible to getting sick.
- We can say with absolute certainty that there is no overwhelming risk. It’s wrong to say the opposite.
- Many doctors are smart but don’t have a huge amount of time to question things. Most doctors get their information in the same way most people do and unfortunately that information has been very biased. The science has moved on but the narrative has not.
- The media was responsible for amplifying the fear about something they didn’t know about.
- Models are useful scientifically when you have an understanding of something but they’re very bad at predicting outcomes. The government should have known this because we’ve have many examples of models and resulting policies being spectacularly wrong.
- Politicians have forgotten that leadership is not about telling people what they want to hear. Where is the criticism of the narrative?
- There is no evidence that lockdown has had any effect except in modelling. The evidence show that the lockdown plays out in similar way.
Professor Karl Friston is a computer modelling expert, world-renowned for his contributions to neuroscience. He has been applying his “dynamic causal modelling” approach to the Covid-19 pandemic, and has reached some startling results.
– The differences between countries are not primarily down to government actions, but due to ‘intrinsic’ differences in the populations
– We don’t yet fully understand what is driving it, although there are theories ranging from levels of vitamin D to genetic differences
– In each country, there appears to be a portion of the population that is ‘not even in the game’ – that is, not susceptible to Covid-19. This varies hugely between countries
– In the UK, Professor Friston estimates that portion to be at least 50%, and probably more like 80%
– The similar mortality results between Sweden (no lockdown) and the UK (lockdown) are best explained by the fact that in reality there was no difference
– the impact of the legal lockdown in Professor Friston’s models “literally goes away”.
Masks and respirators do not work. There have been extensive randomized controlled trial (RCT) studies, and meta-analysis reviews of RCT studies, which all show that masks and respirators do not work to prevent respiratory influenza-like illnesses, or respiratory illnesses believed to be transmitted by droplets and aerosol particles. Furthermore, the relevant known physics and biology, which I review, are such that masks and respirators should not work. It would be a paradox if masks and respirators worked, given what we know about viral respiratory diseases: The main transmission path is long-residence-time aerosol particles (< 2.5 μm), which are too fine to be blocked, and the minimum-infective-dose is smaller than one aerosol particle. The present paper about masks illustrates the degree to which governments, the mainstream media, and institutional propagandists can decide to operate in a science vacuum, or select only incomplete science that serves their interests. Such recklessness is also certainly the case with the current global lockdown of over 1 billion people, an unprecedented experiment in medical and political history.
Update: The researchgate.net link no longer works but an archive on archive.org is available:
Update 2 July 2020: Denis Rancourt talks about his paper in this video.
Update 30 July 2020: Del Bigtree’s channel has been censored by YouTube. His video with Denis Rancourt has been mirrored below.
Pharmaceutical companies are putting pressure on scientific results says Philippe Douste-Blazy, Cardiology MD, Former France Health Minister.
Mirror:
Patients kept waiting for hours secretly record NHS hospital staff doing #TikTok rehearsal.
“That’s why we’ve been waiting so long”
“They are mugging the system”
“Is this really happening? Am I really witnessing this??”
“I’ve seen it all now”
Source: https://t.co/sgI8efmG3I
Podcast highlights
- There were many signs that were really available by the end of February indicating this is a virus that has ‘weak legs.’
- The data was all available by the end of February [2020] and anyone who can use Excel could analyse it.
- “The best statistical test is the eyeball test.” And if you chart things in Excel, you can very quickly make an instinctive judgement.
- No country succeeded in protecting the elderly and nursing homes–it’s hard thing to do.
- We had a soft flu season. The people who would have been susceptible to a generic flu were hit by a virus that came late and swept through rapidly. This could explain the high COVID-19 death numbers among the vulnerable.
- Many analysts agree that the lockdown did nothing to affect the peak of infections and deaths.
- None of the pro-lockdown people seemed to analyse the data and used the data to support lockdown.
- Many pro-lockdown scientific colleagues are academics receiving salaries; their lives would not be negatively affected by the lockdown. Scientists love nothing more than staying at home to work.
- What really matters is the years lost rather than the number of dead. Life is risky and when you’re old, life is more risky. You’re expecting younger people to give their future to get two more months of life.
- While COVID-19 is not the same as the flu, the numbers look very similar.
- People rolled over for a lockdown based on no real solid science.
- There’s a whole fallacy about the R value because it is dependent on the time you’re infected and no one knows what the time infected is, no one knows about hidden cases.
Source website: https://thefatemperor.com
We spoke to Sunetra Gupta, Professor of Theoretical Epidemiology at the University of Oxford and head of the team that released a study in March which speculated that as much as 50% of the population may already have been infected and the true Infection Fatality Rate could be as low as 0.1%.
In her first major interview since the Oxford study was published, she goes further by arguing that Covid-19 has already passed through the population and is now on its way out. She said:
On antibodies:
• Many of the antibody tests are “extremely unreliable”
• They do not indicate the true level of exposure or level of immunity • “Different countries have had different lockdown policies, and yet what we’ve observed is almost a uniform pattern of behaviour”
• “Much of the driving force was due to the build-up of immunity”On IFR:
• “Infection Fatality Rate is less than 1 in 1000 and probably closer to 1 in 10,000.”
• That would be somewhere between 0.1% and 0.01%On lockdown policy:
• Referring to the Imperial model: “Should we act on a possible worst case scenario, given the costs of lockdown? It seems to me that given that the costs of lockdown are mounting that case is becoming more and more fragile”
• Recommends “a more rapid exit from lockdown based more on certain heuristics, like who is dying and what is happening to the death rates”
On the UK Government response:
• “We might have done better by doing nothing at all, or at least by doing something different, which would have been to pay attention to protecting the vulnerable”
On the R rate:
• It is “principally dependent on how many people are immune” and we don’t have that information.
• Deaths are the only reliable measure.
On New York:
• “When you have pockets of vulnerable people it might rip through those pockets in a way that it wouldn’t if the vulnerable people were more scattered within the general population.”On social distancing:
• “Remaining in a state of lockdown is extremely dangerous”
• “We used to live in a state approximating lockdown 100 years ago, and that was what created the conditions for the Spanish Flu to come in and kill 50m people.”On next steps:
• “It is very dangerous to talk about lockdown without recognising the enormous costs that it has on other vulnerable sectors in the population”
• It is a “strong possibility” that if we return to full normal tomorrow — pubs, nightclubs, festivals — we would be fine.On the politics of Covid:
• “There is a sort of libertarian argument for the release of lockdown, and I think it is unfortunate that those of us who feel we should think differently about lockdown”
• “The truth is that lockdown is a luxury, and it’s a luxury that the middle classes are enjoying and higher income countries are enjoying at the expense of the poor, the vulnerable and less developed countries.”