Policy
Browse the articles related to this topic below.
Join our community on Guilded.
- The NHS has not resumed anything like normal service. But the predicted Covid deluge never materialised.
- Current Covid death toll of 41,628 is barely half the total fatalities of the 1968 flu epidemic in the UK.
- Hospital admissions for cancer were down by 36 per cent in April and another 37 per cent in May.
- The State has wildly over-reacted, partly as a result of being in thrall to scientists such as Professor Neil Ferguson with unproven theories and dubious modelling.
- More than 1,600 people die in Britain every day, yet, despite the Government’s scaremongering, the coronavirus daily death toll has been in single or low double figures for weeks.
- The ‘rule of six’ has no scientific evidence to back it up, and may well end up having major social consequences.
- Increased activity at the end of summer leads to an increase in acute respiratory infections, as it does every year.
- Oxford University’s Centre for Evidence Based Medicine: no scientific evidence on the effects of measures such as distancing on respiratory viral spread. No study pointing to the number six. If it’s made up, why not five or seven?
- Admissions for Covid, critical care bed occupancies and deaths are now at an all-time low.
- There are currently 600 patients in hospital with Covid compared to over 17,000 at the height of the epidemic. An average of ten patients a day die with Covid registered on their death certificate, compared to over 1,000 at the peak.
- Shift in focus away from the impact of the disease is a worrying development.
- Severity of the pandemic was monitored by numbers of cases, numbers of admissions, and deaths. All three measures are open to misinterpretation if their definitions are not standardised.
- Cases are being over-diagnosed by a test that can pick up dead viral load.
- Hospital admissions are subjective decisions made by physicians which can vary from hospital to hospital.
- Even deaths have been misattributed.
- Cases will rise, as they will in winter for all acute respiratory pathogens, but this will not necessarily translate into excess deaths.
- Models ignore the vast expertise of our clinicians and public health experts who could provide a more robust approach based on their real-world healthcare experiences.
- The current Cabinet is inexperienced:
- the Health Secretary has been in post for just over two years now;
- the PM and the Chief Medical Officer a year;
- The Joint Biosecurity Centre is overseen by a senior spy who monitors the spread of coronavirus and suppresses new outbreaks;
- New chair of the National Institute for Health Protection who has little or no background in healthcare.
- The recognised alert threshold for ‘regular’ acute respiratory infections is 400 cases per 100,000.
- Britain’s mental health has deteriorated. During lockdown, a fifth of vulnerable people considered self-harming, routine healthcare came to a standstill, operations were cancelled, and cancer care put on hold.
- The most glaring initial blunder was not observing what was going on in other European nations and learning from their mistakes.
- Life should return to as close as possible to normality.
https://www.spectator.co.uk/article/boris-johnson-needs-to-bin-the-rule-of-six
Categories
The future of citizen data systems – GOV.UK
Citizen data is growing rapidly in volume and variety, and is increasingly internationally mobile. This has the potential to bring huge benefits to the economy and society, but also increased risks.
This report examines different approaches to the governance, control and use of citizen data across the world. It aims to inform public debate and government decisions with an international, whole-system view of citizen data. Variations in regional data systems both reflect and determine developments in the economy, security and society.
FORCING school children to wear masks is part of a scattergun approach by a government “lacking the political will” to study the actual evidence, a professor warns.
Dr Carl Heneghan said that the mask doctrine came into place even as the deputy chief medical officer admitted there was no strong evidence they would help with the disease. This was despite the social and psychological damage masking pupils would cause, he said. He pointed out that with drug interventions, high quality testing was required before they were implemented.
…He said: “Wearing masks can interfere with social wellbeing. We clearly understand with drugs the need to do proper research on the benefits against the harms before we use them.
This is a huge intervention to impose on society with many unknowns and potentially damaging consequences, but we are not doing the research to justify it.”
The NHS has a “hidden waiting list” of 15.3 million patients who need follow-up appointments for health problems, according to the first analysis of its kind.
The official waiting list, which stands at 3.9 million, shows how many patients are yet to have their first hospital appointment after a GP referral.
However, the total number who are on hospital books in England and need appointments is not collated centrally. A new calculation, based on freedom of information requests to NHS trusts and seen by The Times, puts the figure at 15.3 million.
Although the official waiting list, after initial referral by a GP, has remained at a fairly stable level throughout the pandemic, this has been mainly driven by fewer patients joining it.
https://www.thetimes.co.uk/article/coronavirus-nhs-data-shows-15m-on-hidden-waiting-list-w250vxvz6
Scores of MPs and former ministers have urged the prime minister to tackle a backlog in NHS cancer care that threatens to lead to thousands of early deaths over the next decade.
One senior oncologist has claimed that in a worst-case scenario the effects of the pandemic could result in 30,000 excess cancer deaths over the next decade.
We have consistently (and I’d say flagrantly) over-estimated the threat of Covid-19, starting with the absurd prediction of 500,000 deaths by Imperial College London’s Professor Neil Ferguson. Data experts who later reviewed the computer code used in the professor’s model described it as “a mess which would get you fired in private industry”…
The trashing of the economy, the worst recession in our history, avoidable deaths at home with people too frightened to go to hospital for fear of catching the virus, chaos in education, the explosion in domestic violence, steep rises in anxiety, depression, and heavy drinking?
No. Lockdown will come to be seen as one of the most catastrophic misjudgments a British government has ever made.
The Imperial College study published this morning claiming that 3.4 million people ( six per cent of the UK population) have antibodies indicating that they have been exposed to Covid-19 provides no great revelation. The Office of National Statistics (ONS) has already published similar figures suggesting that 6.5 per cent of the population has been infected. Nevertheless, it is yet more confirmation of how irrelevant are the official statistics for Covid 19 cases – and what a nonsense it is to rely on them for policymaking.
According to the Government’s Covid “dashboard”, updated at 4pm on Wednesday, 313,798 people in Britain have had the disease. This is less than one tenth of the number suggested by the Imperial study. In other words, for all Matt Hancock’s efforts to ramp up testing, the vast majority of cases have not been detected.
https://www.telegraph.co.uk/news/2020/08/13/massively-overreacting-new-covid-outbreaks/
You may realise my personification of the NHS, referring to it as she and her. Why? Well, the narrative of the NHS is the narrative of all of us. How many of us were born in an NHS hospital? How many of our lives and our family’s lives has she saved? The NHS is more than a set of buildings or a mere organisation; she is every one of us. A living, breathing establishment made up of 1.5 million dedicated workers, 66.6m patients. She is ours, and we are hers.
Lockdowns may reduce the peak of transmission and recovery rates but not the number of critical cases or overall mortality.
Lastly, government actions such as border closures, full lockdowns, and a high rate of COVID-19 testing were not associated with statistically significant reductions in the number of critical cases or overall mortality.
…full lockdowns and early border closures may lessen the peak of transmission, and thus prevent health system overcapacity, which would facilitate increased recovery rates.
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(20)30208-X/fulltext
This recent crop of trials added 9,112 participants to the total randomised denominator of 13,259 and showed that masks alone have no significant effect in interrupting the spread of ILI or influenza in the general population, nor in healthcare workers.
The small number of trials and lateness in the pandemic cycle is unlikely to give us reasonably clear answers and guide decision-makers. This abandonment of the scientific modus operandi and lack of foresight has left the field wide open for the play of opinions, radical views and political influence.
https://www.cebm.net/covid-19/masking-lack-of-evidence-with-politics/
2:55 – Masks
• Tom Jefferson: “Aside from people who are exposed on the frontlines, there is no evidence that masks make any difference, but what’s even more extraordinary is the uncertainty: we don’t know if these things make any difference…. We should have done randomised control trials in February, March and April but not anymore because viral circulation is low and we will need huge number of enrolees to show whether there was any difference”.
• Carl Heneghan: “By all means people can wear masks but they can’t say it’s an evidence-based decision… there is a real separation between an evidence-based decision and the opaque term that ‘we are being led by the science’, which isn’t the evidence”.
9:26 – Pandemic life cycle
• CH: “One of the keys of the infection is to look at who’s been infected, which shows a crucial difference when comparing the pandemic theory to seasonal theory. In a pandemic you’d expect to see young people disproportionately affected, but in the UK we’ve only had six child deaths, which is far less than we’d normally see in a pandemic. The high number of deaths with over-75s fits with the seasonal theory”.
14:00 – Covid seasonality
• CH: “The stability of the virus is far less when the temperature goes up but humidity seems to be particularly important. The lower the humidity, the more stable the virus is in the atmosphere and on surfaces… It’s now winter in the southern hemisphere, which is why places like Australia are suddenly having outbreaks.”
20:37 – Lockdown
• CH: “Many people said that we should have locked down earlier, but 50% of care homes developed outbreaks during the lockdown period so there are issues within the transmission of this virus that are not clear… Lockdown is a blunt tool and there needs to be intelligent conversations about what mitigation strategies can keep society functioning while we keep the most vulnerable shielded”.
25:20 – Nightingale hospitals
• CH: “They are the wrong structure. What you need is fever hospitals which were here until around the 1980s or 90s. They were on single floors and had isolation within isolation. Theere were no lift shafts and staff were trained, which meant that everyone was protected from each other… It looks like at leats 20% of people got the infection while they were in hospital”
27:30 – Suppression strategy
• CH: “The benefits of the current strategy are outweighed by the harms…When it comes to suppression, only the virus will have a determination in that. If you follow the New Zealand policy of suppressing it to zero and locking down the country forever, then you’re going to have a problem… This virus is so out there now, I cannot see a strategy that makes suppression the viable option. The strategy right now should be how we learn to live with this virus”
32:45 – Response to the virus
• TJ: “I am a survivor of four pandemics and for the other three, I didn’t even realise they were going on. People died but nothing changed and none of the fabric of society was eroded like this response… Do I see steps being taken at a European level about learning from our mistakes and changing policies? The answer is no…
39:30 – Politics of the virus
• CH: “We as individuals are part of the problem because sensationalism drives people to click and read the information. So it’s a big circle because we’ve created the problem — if we put the worst case scenario out there, we will go and have a look. If you want a solution, you’ve got to get people to stop clicking on this sensationalist stuff”.
43:30 – IFR
• CH: “We will be down about where we were with the swine flu: around 0.1-0.3% which is much lower than what we think because at the moment we are seeing the case fatality”.
• TJ: “If you look at the whole narrative, it was distorted from the very beginning by the obsession with influenza which was just one or two agents and nothing else existed. We’re no different now”.
Increasing COVID-19 caseloads were associated with countries with higher obesity (adjusted rate ratio [RR]=1.06; 95%CI: 1.01–1.11), median population age (RR=1.10; 95%CI: 1.05–1.15) and longer time to border closures from the first reported case (RR=1.04; 95%CI: 1.01–1.08). Increased mortality per million was significantly associated with higher obesity prevalence (RR=1.12; 95%CI: 1.06–1.19) and per capita gross domestic product (GDP) (RR=1.03; 95%CI: 1.00–1.06). Reduced income dispersion reduced mortality (RR=0.88; 95%CI: 0.83–0.93) and the number of critical cases (RR=0.92; 95% CI: 0.87–0.97). Rapid border closures, full lockdowns, and wide-spread testing were not associated with COVID-19 mortality per million people. However, full lockdowns (RR=2.47: 95%CI: 1.08–5.64) and reduced country vulnerability to biological threats (i.e. high scores on the global health security scale for risk environment) (RR=1.55; 95%CI: 1.13–2.12) were significantly associated with increased patient recovery rates.
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(20)30208-X/fulltext
- Some experts argued that masks would help slow the infection rate.
- Others pointed out that improper use of face masks can amplify risks, for instance by acting as a reservoir for virus particles.
- It seems that today’s mantra of ‘listen to the science’ is not as straightforward as it seems.
- Claims to wear masks are untested and unchallenged, then elevated to the status of ‘the science’.
- The hasty assembling of research articles in support of a policy position is not science. This is as likely to be to be dangerously misleading as it is to yield even negligible benefits.
- Scientific controversy in the 21st century is settled by institutional weight and muscle, not by experiment.
- The president of the Royal Society wants to have his cake and eat it: he wants the government to defer to institutional science, but not for science to be accountable for this influence.
- The government, weakened by its capitulations to breakfast TV anchors, politically motivated scientists and scientific institutions, may find itself unable to roll back policies which turn out to do more harm than good.
https://www.spiked-online.com/2020/07/16/the-government-has-lost-control/
- From late-February 2020, Birmingham City Council gave care homes a £1,000 extra cash to take in hospital patients in a hurry, including some with coronavirus.
- Reason: more NHS beds could be freed up for coronavirus patients.
- Care home had to bid for the resident in a four hour window and, if their bid was ‘winning’, organise admission within 24 hours – regardless of the citizen’s Covid-19 testing or diagnosis status at the point of discharge.
- Care home manager, Jane Farr, of Digby Manor care home in Erdington, believes her rejection of the offer is one of the reasons none of her residents have been infected.
- From late February, any in-patients deemed ‘fit to discharge’ were rapidly moved out of hospital so hospital staff could focus on coronavirus patients.
- Dr David Rosser, chief executive of University Hospitals Birmingham (UHB) said the city created too much capacity – indicating some of the frantic measures to empty beds turned out to be not needed.
- From April 15 the Government’s rules changed and all discharged residents were supposed to undergo a test first.
https://www.birminghammail.co.uk/news/midlands-news/revealed-16-care-homes-given-18550503
The new Oxford study released by Royal Society and British Academy does not prove face coverings work. It is a policy document masquerading as an investigation into face coverings.
The Mayor Of London claims new evidence supports the use of face coverings as effective in reducing the spread of COVID-19. He cites a University of Oxford study that claims: “face masks and coverings work – act now.“
The study, from Oxford’s Leverhulme Centre for Demographic Science, is freely available for download from The Royal Society website. Nevertheless, we doubted that many people would take time to verify the claims so we took a look. What did we find?
The bulk of study is in fact an investigation into policies and behavioural factors behind face mask usage. Only a small section is dedicated to analysing the effectiveness of cloth face coverings and even this provides nothing new. Further, rather than performing randomised controlled trials (RCTs), which form the highest level of evidence in medical science, this report simply looked at existing research.
From this existing research, the authors forced a conclusion that ‘face masks and coverings work’ but with some very important caveats:
- The tests were carried out in medical and lab settings, not within the community.
- There were other factors that contributed to the masks’ effectiveness.
- The conclusions were based on small studies.
The study limitations can be found in the document appendix, table A5.1.

What can we conclude from the release of this study?
It seems evidence for universal masking of healthy people in the community so flimsy that sleight of hand is needed in order to push public acceptance.
Update 19 July 2020:
A Spiked Online article published on 16 July, The government has lost control, draws the same conclusions:
The Royal Society published, on 26 June, a ‘rapid review of the science of the effectiveness of different face-mask types’ – a dense, 37-page tract which made the case for face masks. It was neither peer-reviewed nor opened to wide expert and public debate before being used to argue for policy.
…the hasty assembling of research articles in support of a policy position is not science, and demanding that the government introduce new ‘taboos’ is naive and clumsy social engineering, not careful examination of the facts.
Such is the quality of decision-making in the process generating our lockdown narrative. An early maintained but exaggerated belief in the lethality of the virus reinforced by modelling that was almost data-free, then amplified by further modelling with no proven predictive value. All summed up by recommendations from a committee based on qualitative data that hasn’t even been peer-reviewed.
- According to Office for National Statistics, this year comes only eighth in terms of deaths in past 27 years.
- The spread of viruses like Covid-19 is not new. What’s new is our response.
- The whole Covid drama has really been a crisis of awareness of what viruses normally do, rather than a crisis caused by an abnormally lethal new bug.
- Modelling is not science, for the simple reason that a prediction made by a scientist (using a model or not) is just opinion.
- To be classified as science, a prediction or theory needs to be able to be tested, and potentially falsified.
- A problem with the current approach: a wilful determination to ignore the quality of the information being used to set Covid policy.
- Most Covid research was not peer- reviewed.
- In medical science there is a well-known classification of data quality known as ‘the hierarchy of evidence’: a seven-level system gives an idea of how much weight can be placed on any given study or recommendation.
- Randomised controlled trials (RCTs) form the highest, most reliable form of medical evidence: Level 1 and 2.
- Virtually all evidence pertaining to Covid-19 policy is found in the lowest levels (much less compelling Levels 5 and 6): descriptive-only studies looking for a pattern, without using controls.
- Level 7 is at the bottom of the hierarchy (the opinion of authorities or reports of expert committees) because ‘authorities’ often fail to change their minds in the face of new evidence.
- Committees often issue compromise recommendations that are scientifically non-valid.
- The advice of Sage (or any committee of scientists) is the least reliable form of evidence there is.
https://www.spectator.co.uk/article/how-strong-was-the-scientific-advice-behind-lockdown

COVID-19 started registering with most of the British public around late February and early March. Many were concerned but not particularly afraid. Only weeks later people were terrified to leave their homes or go near other human beings. How did such a dramatic shift in public perception happen so quickly?
In early March 2020, The Scientific Advisory Group for Emergencies (SAGE) produced a document for the UK Government highlighting methods for rolling out new social distancing rules. There seemed to be some doubt as to whether the public would comply with the upcoming measures so SAGE outlined a methodology based on known psychological behavioural modification techniques.
SAGE, SPI-B and applied psychology
SAGE is an advisory group to the UK government responsible for making sure decision makers have access to scientific advice. We are told that the advice provided by SAGE does not represent official government policy.
SAGE also relies on expert sub-groups for COVID-19 specific advice. These sub-groups include:
- NERVTAG: New and Emerging Respiratory Virus Threats Advisory Group
- SPI-M: Scientific Pandemic Influenza Group on Modelling
- SPI-B: Independent Scientific Pandemic Influenza Group on Behaviours
The identity of individual committee members themselves were initially kept secret, purportedly due to national security. Some names were eventually released, largely due to efforts by UK businessman Simon Dolan and his legal challenge campaign. Nevertheless, two members remain anonymous.
Psychological techniques for behavioural change
The document itself, titled Options for increasing adherence to social distancing measures, was drafted by SPI-B, the behavioural science sub-group for SAGE.
SPI-B highlighted nine broad ways of achieving behavioural change in the public:
- Education
- Persuasion
- Incentivisation
- Coercion
- Enablement
- Training
- Restriction
- Environmental restructuring
- Modelling
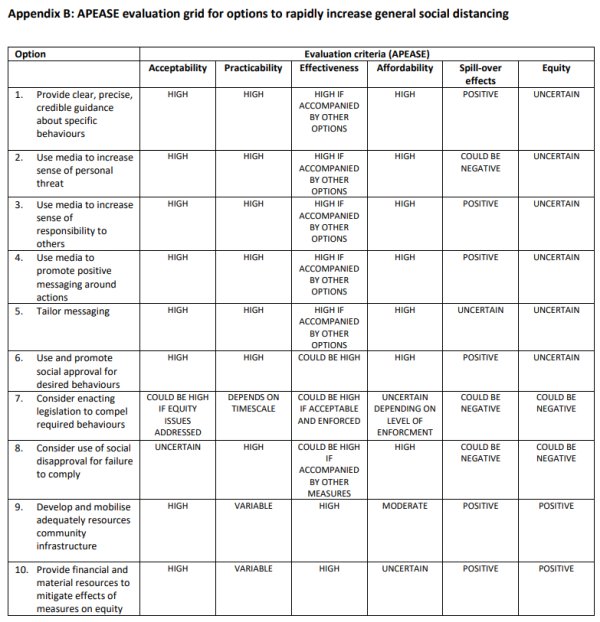
In the document, SPI-B focused on the methods most relevant to their stated goals and set out ten options that were evaluated on six criteria.
The six criteria, under the acronym APEASE, were:
- Acceptability
- Practicability
- Effectiveness
- Affordability
- Spill-over effects
- Equity
Government persuasion through fear
A key part of SPI-B’s behavioural change strategy that seems to have been adopted was to ‘persuade through fear.’ The Persuasion section of the document states:
A substantial number of people still do not feel sufficiently personally threatened.
Clearly, the psychologists felt that, as of late March, the public was still not afraid of COVID-19. It therefore suggested that the government increase the level of fear:
The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging.
Appendix B of the document lists ten options that can be used to increase social distancing in the public. Option 2 advises:
Use media to increase sense of personal threat.
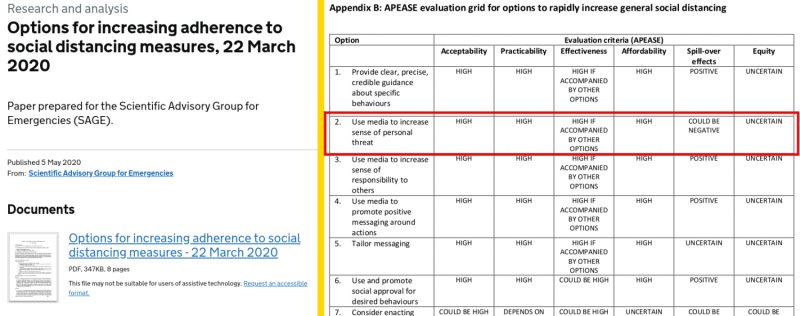
In hindsight, this explains the tone of government sponsored social media and physical billboard advertising campaigns that started appearing around April.
SPI-B recommendations to increase personal threat and use hard-hitting emotional messaging are on display with eerie imagery coupled with taglines such as:
- “Anyone can get it. Anyone can spread it.“
- “Don’t put your friends and family in danger.“
- “Stay home for your family. Don’t put their lives in danger.“
- “If you go out, you can spread it. People will die.“


Hysterical news headlines
During the first week of April 2020, the InProportion2 project noticed a change in the BBC headlines and posted the article, BBC: Informing or scaring?
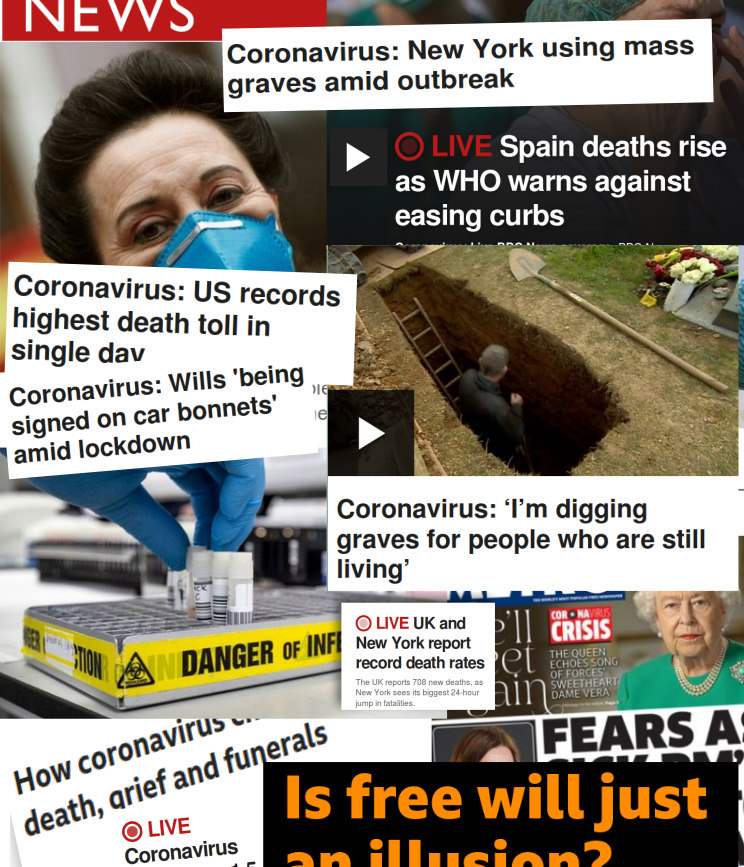
The article compared hysterical BBC news headline from the first week of April 2020 with those from 2018, when mortality rates were peaking due to a bad flu season. It found no references to flu or excess mortality on the BBC home page during the 2018 peak. InProportion2 asked, “Do the headlines reflect the gravity of the situations in an equivalent way – or is additional fear being stirred up in 2020?“
Persuasion through shame and approval: Covidiots and heroes
SPI-B psychologists knew that fear on its own would not persuade everyone. Messaging needed to be tailored to take into account different ‘motivational levers.’
Some people will be more persuaded by appeals to play by the rules, some by duty to the community, and some to personal risk.
It therefore suggested using both social approval and disapproval, with compulsion (legislation) as a backup:
- Option 6: Use and promote social approval for desired behaviours
- Option 7: Consider enacting legislation to compel required behaviours
- Option 8: Consider use of social disapproval for failure to comply
We can see the obvious approval-disapproval dialectic with the ‘Heroes and Covidiots’ narrative that soon began to surface in the news. The term ‘Covidiot’ appeared around March with The Economist’s 1843 Magazine describing covidiots in this way:
Even in a pandemic, many of us are prone to judge others and find them wanting: the term “covidiot” describes any and every person behaving stupidly or irresponsibly as the epidemic spreads. Sometime in early March the word was born, and, almost as fast as the virus spread, so did instances of covidiotic behaviour.
Although it’s not clear how the term came about, it was quickly adopted in UK mainstream and social media. At the same time, we began seeing praise for heroes who ‘did the right thing’ by complying with the government measures.
The METRO article below shows all three options in play:
- Social approval: “These local heroes have been doing amazing things…”
- Social disapproval: “Lake District closed…because covidiots won’t stay away…”
- Compulsion: “Matt Hancock threatens to close beaches…”

An incentivised media
These psychological techniques would have been impossible to deploy on the public without a compliant media. How did the government convince the media to go along with the plan?
Increased UK government media spending
Digiday, a media and marketing industry publication, reported in April that the government is becoming UK news publishers’ most important client. In the 20 April 2020 article for Digiday, Lara O’Reilly wrote:
…the government is spending more than usual, judging by their bookings. The publishers also pointed out that the lack of activity from other advertisers in the current market means the government campaigns will have an outweighed share of voice compared with normal times.

During that period, the British public started seeing coverage across media outlets with the unified “In this together” messaging. O’Reilly pointed out that the campaign was worth £35 million over a three month period.
Last week, the government and newspaper industry launched a three-month advertising partnership dubbed “All in, all together.” The campaign — worth approximately £35 million ($44 million) for the full course, according to sources — kicked off on Apr. 17, with all the U.K.’s national and regional daily news brands running near-identical cover wraps and homepage takeovers, which carried the copy, “Stay at home for the NHS, your family, your neighbours, your nation the world and life itself.”
So, we ask again: how did the government convince the media to go along with the plan? The answer is simple and obvious: with lots of money.
Psychological techniques to change behaviour
We can see that the UK Government has a public document outlining psychological techniques to change the behaviour of the population. We see a unified mass-media campaign that falls in line with these techniques. We then see a dramatic shift in public perception and behaviour.
What else can we call this but ‘brainwashing’?
Despite the open nature of what has transpired, it seems to have gained little coverage in the media. This is of no surprise since it was clearly complicit in spreading fear in the public.
Download the document
The document is freely downloadable on the gov.uk website in a page titled, “Research and analysis – Options for increasing adherence to social distancing measures, 22 March 2020“.
We encourage you to read the document, compare it with your observations about how the government and media has acted, then make up your own mind.
Updates
March 2023:
Leaked messages revealed by The Telegraph proved that Matt Hancock and other UK government ministers planned to “frighten the pants off” the public and ensure they complied with lockdown.
January 2021:
After seven months the mainstream media finally catches up. On 24th January 2021, The Express published the following article: Government accused of using Covid fear tactics to inflate anxiety levels of British public.
March 2021:
- Campaign, the world’s leading business media brand for the marketing and advertising, reported that the UK government spent more than £184m on Covid communications in 2020.
- It has emerged that German politicians, scientists and public health bureaucrats have also collaborated to induce panic to justify the first German lockdown. The source material is in German but a Twitter thread explaining the leaks in English has been archived. We will update here if an English source becomes available.
- On 18 March, the UK Government put out a tender for a £2m COVID Public Information Campaign for Northern Ireland. It is to last to years starting 1 April 2021.
- In an article for the Critic, A year of fear, Dr. Gary Sidley wrote about the role of SPI-B and The Behavioural Insights Team in bombarding the British public with fear-inducing information. Dr. Sidley is a member of the Health Advisory and Recovery Team.
April 2021:
- The mainstream media is now acknowledging the government’s psychological strategies to manipulate behaviour of the British public. On 2 April, The Telegraph published the article, State of fear: how ministers ‘used covert tactics’ to keep scared public at home.
- The UK Cabinet Office awarded £320,000,000 for COVID 19 – Media Buying Services in advertising, radio and television. The contract runs between 1st April 2021 to 31 March 2022. See our archive of UK Government COVID-19 media buying.
May 2021:
- Researcher Ian Davis reports about the ties between the UK Government and Omnicom, the New York-based corporate communications company the behind the phrases “flatten the curve”, “stay home, protect the NHS, save lives”, “rule of six” and “look into my eyes” campaigns. The UK Government has awarded Omnicom with £1.6 billion in media buy-in contracts since 2018.
- On 14th May 2020, The Telegraph published an article of SPI-B members admitting that the Use of fear to control behaviour in Covid crisis was ‘totalitarian’.
- Author, journalist, photographer and filmmaker Laura Dodsworth released her new book, A State of Fear: how the UK government weaponised fear during the Covid-19 pandemic, on 17th May 2021.
A State of Fear:
Laura Dodsworth talks about her book State of Fear on The James Delingpole Channel.
Update 27 June 2020: For a more in-depth commentary, please read How SAGE and the UK media created fear in the British public
In early March 2020, The Scientific Advisory Group for Emergencies (SAGE) produced a document for the UK Government highlighting recommendations for increasing adherence to social distancing measures. There seemed to be some doubt as to whether the public would comply with the upcoming measures so SAGE developed a methodology based on criteria called ‘APEASE’.
The document itself was drafted by SPI-B, the behavioural science sub-group for SAGE. More information about SPI-B can be found in this document.
APEASE criteria
In the document, behavioural change options were set in a grid and evaluated based on the six criteria. See Appendix B in the linked document.
SPI-B’s APEASE criteria are:
- Acceptability
- Practicability
- Effectiveness
- Affordability
- Spill-over effects
- Equity
Persuasion through fear
It seems that a big part of SPI-B’s behavioural change strategy was to ‘persuade through fear.’ The Persuasion section of the document states:
The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging. To be effective this must also empower people by making clear the actions they can take to reduce the threat.
Appendix B of the document lists ten options that can be used to increase social distancing in the public. Option 2 advises: “Use media to increase sense of personal threat.“
Psychological techniques to change behaviour
In this document, the UK Government has openly admitted to using psychological techniques to change the behaviour of the British population. Despite the open nature of this admission, it seems to have gained little coverage in the media.
This is of no surprise since the British media was clearly complicit in spreading fear in the public.
Download the document
The document is freely downloadable on the gov.uk website in a page titled, “Research and analysis – Options for increasing adherence to social distancing measures, 22 March 2020“.