Financial incentives and conflicts of interest have been revealed throughout the COVID-19 crisis. Hospitals were offered extra funding for each COVID-19 patient. Care homes were paid to accept patients discharged from hospital regardless of the testing or diagnosis status.
Little is known about the interests of the doctors, scientists, and academics on whose advice the UK government relies to manage the pandemic. Attempts to discover more are frequently thwarted, finds Paul D Thacker.
Politicians and governments are suppressing science. They do so in the public interest, they say, to accelerate availability of diagnostics and treatments. They do so to support innovation, to bring products to market at unprecedented speed. Both of these reasons are partly plausible; the greatest deceptions are founded in a grain of truth. But the underlying behaviour is troubling.
Politicians and governments are suppressing science. They do so in the public interest, they say, to accelerate availability of diagnostics and treatments. They do so to support innovation, to bring products to market at unprecedented speed. Both of these reasons are partly plausible; the greatest deceptions are founded in a grain of truth. But the underlying behaviour is troubling.
Politicians and governments are suppressing science. They do so in the public interest, they say, to accelerate availability of diagnostics and treatments. They do so to support innovation, to bring products to market at unprecedented speed. Both of these reasons are partly plausible; the greatest deceptions are founded in a grain of truth. But the underlying behaviour is troubling.
The UK’s pandemic response provides at least four examples of suppression of science or scientists. First, the membership, research, and deliberations of the Scientific Advisory Group for Emergencies (SAGE) were initially secret until a press leak forced transparency.2 The leak revealed inappropriate involvement of government advisers in SAGE, while exposing under-representation from public health, clinical care, women, and ethnic minorities. Indeed, the government was also recently ordered to release a 2016 report on deficiencies in pandemic preparedness, Operation Cygnus, following a verdict from the Information Commissioner’s Office.
Practices will be paid £12.58 (€14.15; $16.69) per vaccination. This is 25% more than the current £10.06 practices receive for an influenza vaccination, in recognition of the need for extra training, post-vaccine observation, and other associated costs. Practices will need to provide most of the required staff from their own workforce.
The Cabinet Office signed the lucrative contract with London-based OMD Group as the Government began to gear up its response to the crisis.
Ministers struck a deal worth up to £119m with one of the world’s biggest marketing companies for a Covid campaign three weeks before the country went into a national lockdown, official filings show.
This week, the government promised a total of £1 billion in financial support to local authorities under the new three-tier lockdown system. Areas subjected to Tier 2 lockdowns will be granted £1 per head of the population, and £2 per head for Tier 3. Meanwhile, £30million has been earmarked for local authorities to pay for Covid marshals and other ‘compliance and enforcement’ activities.
Recently, the Government agreed a £161 million deal with a British company called DnaNudge to provide 5.8 million Covid tests, as part of its “Moonshot” programme for mass testing of the population at the point of care. The CovidNudge test is “a rapid, accurate, portable and lab-free RT-PCR test that delivers results at the point of need and in just over an hour”, according to DnaNudge’s own promotional material. DnaNudge is a spinoff company of Imperial College London.
Care home chiefs fear deadly mistakes made at the peak of the coronavirus pandemic risk being repeated as councils offer them extra cash to take Covid-positive hospital patients.
…Now, despite a Government pledge to place a ‘protective ring’ around vulnerable residents, care homes in Cumbria are being offered £1,500 – double the local weekly fee – to take Covid-positive patients from hospital.
…Tony Carling, a care home operator in Cumbria, has decided not to take Covid-positive patients, but fears it could be a costly move. He said: ‘The majority of our clients are funded by local authorities, so it’s very difficult to turn down. You are under extreme financial pressure as to whether you get further business from that authority if you don’t support their needs.’
The UK’s chief scientific adviser has a £600,000 shareholding in a drugs giant contracted to develop a Covid-19 vaccine for the Government, prompting claims of a potential conflict of interest.
Sir Patrick Vallance, Chief Scientific Adviser to UK Government, was president of GSK 2012 – 2018
Holds a deferred bonus of 43,111 shares worth £600,000
Cashed in more than £5m worth of shares upon resignation of GSK
The industry’s awareness that recycling wouldn’t keep plastic out of landfills and the environment dates to the program’s earliest days, we found. “There is serious doubt that [recycling plastic] can ever be made viable on an economic basis,” one industry insider wrote in a 1974 speech.
Drugs are a risky business and, for equity investors hoping to eventually share in the profits, each stage of development presents an escalated risk. Lo reasoned that substantially lowering the risks, even if it meant correspondingly lowering the rewards, could attract investment instead from ordinary bond markets—that is, from managers of pension funds, university endowments, and sovereign-wealth funds, who control a great deal of money and generally invest in low-risk, low-return assets.
Given how uncertain vaccine markets are, the paper notes, governments (“public-sector interventions,” and so forth), would need to guarantee a vaccine bond by committing in advance to purchase and stockpile vaccines. The paper’s most creative suggestion is for a subscription model, a kind of vaccine Netflix, where governments would pay an annual fee to a new international-development fund, one that could perhaps be managed by the G7. The fund could float a bond to both advance vaccine biotechs and to make market commitments to Big Pharma. The virus, the markets, and the science are global.
…it would be much better for the government to say that the money is not from taxpayers. “We’re borrowing it from the rest of the world. And if and when you succeed, or any of the other hundred and fifty projects—that could have been funded, but aren’t being funded right now—succeeds, all the bond holders will get paid. That would be great. Everybody earns a return.”
From late-February 2020, Birmingham City Council gave care homes a £1,000 extra cash to take in hospital patients in a hurry, including some with coronavirus.
Reason: more NHS beds could be freed up for coronavirus patients.
Care home had to bid for the resident in a four hour window and, if their bid was ‘winning’, organise admission within 24 hours – regardless of the citizen’s Covid-19 testing or diagnosis status at the point of discharge.
Care home manager, Jane Farr, of Digby Manor care home in Erdington, believes her rejection of the offer is one of the reasons none of her residents have been infected.
From late February, any in-patients deemed ‘fit to discharge’ were rapidly moved out of hospital so hospital staff could focus on coronavirus patients.
Dr David Rosser, chief executive of University Hospitals Birmingham (UHB) said the city created too much capacity – indicating some of the frantic measures to empty beds turned out to be not needed.
From April 15 the Government’s rules changed and all discharged residents were supposed to undergo a test first.
COVID-19 started registering with most of the British public around late February and early March. Many were concerned but not particularly afraid. Only weeks later people were terrified to leave their homes or go near other human beings. How did such a dramatic shift in public perception happen so quickly?
In early March 2020, The Scientific Advisory Group for Emergencies (SAGE) produced a document for the UK Government highlighting methods for rolling out new social distancing rules. There seemed to be some doubt as to whether the public would comply with the upcoming measures so SAGE outlined a methodology based on known psychological behavioural modification techniques.
SAGE, SPI-B and applied psychology
SAGE is an advisory group to the UK government responsible for making sure decision makers have access to scientific advice. We are told that the advice provided by SAGE does not represent official government policy.
SAGE also relies on expert sub-groups for COVID-19 specific advice. These sub-groups include:
NERVTAG: New and Emerging Respiratory Virus Threats Advisory Group
SPI-M: Scientific Pandemic Influenza Group on Modelling
SPI-B: Independent Scientific Pandemic Influenza Group on Behaviours
The identity of individual committee members themselves were initially kept secret, purportedly due to national security. Some names were eventually released, largely due to efforts by UK businessman Simon Dolan and his legal challenge campaign. Nevertheless, two members remain anonymous.
Psychological techniques for behavioural change
The document itself, titled Options for increasing adherence to social distancing measures, was drafted by SPI-B, the behavioural science sub-group for SAGE.
SPI-B highlighted nine broad ways of achieving behavioural change in the public:
Education
Persuasion
Incentivisation
Coercion
Enablement
Training
Restriction
Environmental restructuring
Modelling
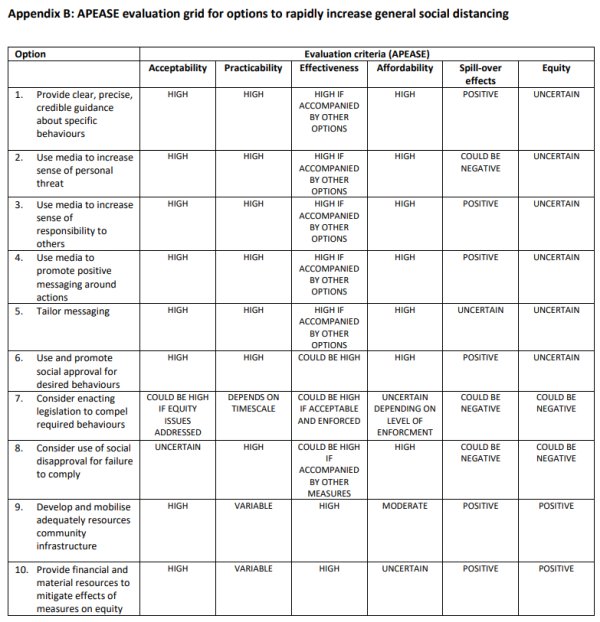
In the document, SPI-B focused on the methods most relevant to their stated goals and set out ten options that were evaluated on six criteria.
A key part of SPI-B’s behavioural change strategy that seems to have been adopted was to ‘persuade through fear.’ The Persuasion section of the document states:
A substantial number of people still do not feel sufficiently personally threatened.
Clearly, the psychologists felt that, as of late March, the public was still not afraid of COVID-19. It therefore suggested that the government increase the level of fear:
The perceived level of personal threat needs to be increased among those who are complacent, using hard-hitting emotional messaging.
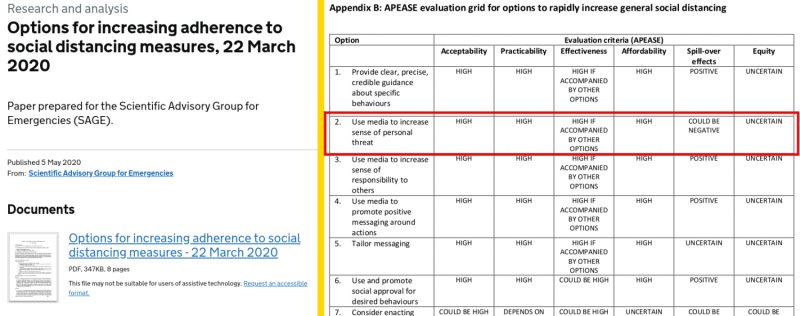
Appendix B of the document lists ten options that can be used to increase social distancing in the public. Option 2 advises:
In hindsight, this explains the tone of government sponsored social media and physical billboard advertising campaigns that started appearing around April.
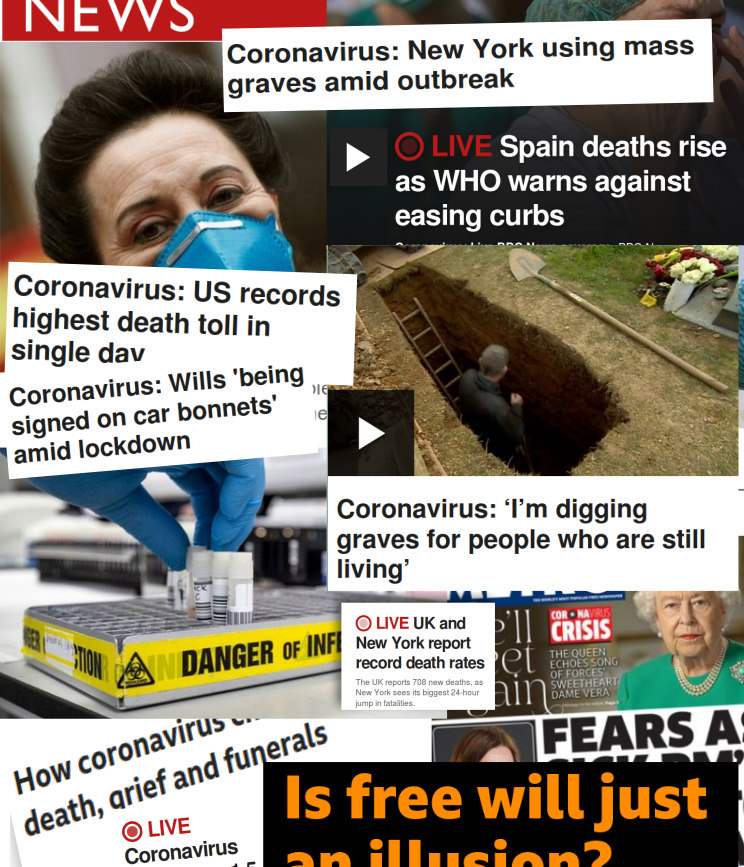
SPI-B recommendations to increase personal threat and use hard-hitting emotional messaging are on display with eerie imagery coupled with taglines such as:
“Anyone can get it. Anyone can spread it.“
“Don’t put your friends and family in danger.“
“Stay home for your family. Don’t put their lives in danger.“
“If you go out, you can spread it. People will die.“
Source: BBC headlines in April 2020 compiled by InProportion2
The article compared hysterical BBC news headline from the first week of April 2020 with those from 2018, when mortality rates were peaking due to a bad flu season. It found no references to flu or excess mortality on the BBC home page during the 2018 peak. InProportion2 asked, “Do the headlines reflect the gravity of the situations in an equivalent way – or is additional fear being stirred up in 2020?“
Persuasion through shame and approval: Covidiots and heroes
SPI-B psychologists knew that fear on its own would not persuade everyone. Messaging needed to be tailored to take into account different ‘motivational levers.’
Some people will be more persuaded by appeals to play by the rules, some by duty to the community, and some to personal risk.
It therefore suggested using both social approval and disapproval, with compulsion (legislation) as a backup:
Option 6: Use and promote social approval for desired behaviours
Option 7: Consider enacting legislation to compel required behaviours
Option 8: Consider use of social disapproval for failure to comply
We can see the obvious approval-disapproval dialectic with the ‘Heroes and Covidiots’ narrative that soon began to surface in the news. The term ‘Covidiot’ appeared around March with The Economist’s 1843 Magazinedescribing covidiots in this way:
Even in a pandemic, many of us are prone to judge others and find them wanting: the term “covidiot” describes any and every person behaving stupidly or irresponsibly as the epidemic spreads. Sometime in early March the word was born, and, almost as fast as the virus spread, so did instances of covidiotic behaviour.
Although it’s not clear how the term came about, it was quickly adopted in UK mainstream and social media. At the same time, we began seeing praise for heroes who ‘did the right thing’ by complying with the government measures.
The METRO article below shows all three options in play:
Social approval: “These local heroes have been doing amazing things…”
Social disapproval:“Lake District closed…because covidiots won’t stay away…”
Compulsion: “Matt Hancock threatens to close beaches…”
These psychological techniques would have been impossible to deploy on the public without a compliant media. How did the government convince the media to go along with the plan?
…the government is spending more than usual, judging by their bookings. The publishers also pointed out that the lack of activity from other advertisers in the current market means the government campaigns will have an outweighed share of voice compared with normal times.
During that period, the British public started seeing coverage across media outlets with the unified “In this together” messaging. O’Reilly pointed out that the campaign was worth £35 million over a three month period.
Last week, the government and newspaper industry launched a three-month advertising partnership dubbed “All in, all together.” The campaign — worth approximately £35 million ($44 million) for the full course, according to sources — kicked off on Apr. 17, with all the U.K.’s national and regional daily news brands running near-identical cover wraps and homepage takeovers, which carried the copy, “Stay at home for the NHS, your family, your neighbours, your nation the world and life itself.”
So, we ask again: how did the government convince the media to go along with the plan? The answer is simple and obvious: with lots of money.
Psychological techniques to change behaviour
We can see that the UK Government has a public document outlining psychological techniques to change the behaviour of the population. We see a unified mass-media campaign that falls in line with these techniques. We then see a dramatic shift in public perception and behaviour.
What else can we call this but ‘brainwashing’?
Despite the open nature of what has transpired, it seems to have gained little coverage in the media. This is of no surprise since it was clearly complicit in spreading fear in the public.
Campaign, the world’s leading business media brand for the marketing and advertising, reported that the UK government spent more than £184m on Covid communications in 2020.
It has emerged that German politicians, scientists and public health bureaucrats have also collaborated to induce panic to justify the first German lockdown. The source material is in German but a Twitter thread explaining the leaks in English has been archived. We will update here if an English source becomes available.
On 18 March, the UK Government put out a tender for a £2m COVID Public Information Campaign for Northern Ireland. It is to last to years starting 1 April 2021.
Researcher Ian Davis reports about the ties between the UK Government and Omnicom, the New York-based corporate communications company the behind the phrases “flatten the curve”, “stay home, protect the NHS, save lives”, “rule of six” and “look into my eyes” campaigns. The UK Government has awarded Omnicom with £1.6 billion in media buy-in contracts since 2018.
The Recovery trial has steadfastly ignored Professor Didier Raoult and a string of countries that have implemented his protocol, early use of HCQ with Azythromycin in safe doses, despite the fact that, after treating 3,737 patients — the single largest study in the world —Raoult has lost only 0.6 per cent, while Horby and Landray are presiding over carnage —a fatality rate of 25 per cent.
The Recovery trial has steadfastly ignored Professor Didier Raoult in the early use of HCQ with Azythromycin in safe doses.
Raoult has lost only 0.6 per cent, while Horby and Landray are presiding over carnage —a fatality rate of 25 per cent.
Landray admitted to an investigative journalist at FranceSoir ‘these are quite high doses to… have a chance of killing the virus.’ Or killing the patient.
Recovery is not the only trial delivering dangerously elevated doses of HCQ to Covid patients. Dosage in the international Solidarity trial was four times greater than the dose being used in India.
WHO has been working for years with Gilead Sciences trying to get the pharmaceutical company’s lacklustre drug Remdesivir to show efficacy at curing first Ebola, with poor results, and now Covid-19.
Landray revealed Gilead pays scientists 20 to 50 times more to conduct a clinical trial than Horby and Landray were paid to conduct the Recovery trial.
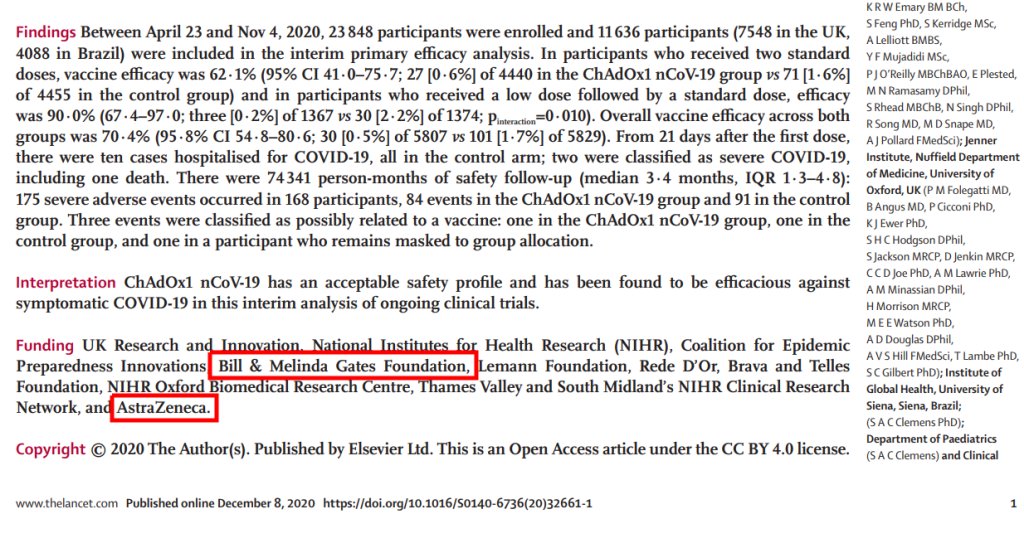
Horby is the executive director of the International Severe Acute Respiratory and Emerging Infection Consortium which received 4.5 million pounds for research into vaccines.
Horby established the Epidemic Research Group which is promised up to 14 million pounds from AstraZeneca and Zuckerberg/Chan of Facebook fame for the development of a Covid-19 vaccine which is being trialled by Oxford University.
AstraZeneca is interested in merging with Gilead Sciences, which, if it went through, would create the biggest Big Pharma ever.
Horby and Landray have announced that dexamethasone, a low-cost steroid which is also being tested has reduced the mortality rate of Covid-19 patients on ventilators from a scandalous 41 per cent to a still appalling 32 per cent.
Raoult has pointed out that in his hospital, of the 0.6 per cent who die, a mere 16 per cent were in ICU
In Britain, where almost 42,000 people have died of Covid, the only thing randomised, controlled trials have achieved, is to blind people to the evidence that 40,000 of those deaths could have been avoided.
According to the president, the World Bank has showed interest in Belarus’ coronavirus response practices. “It is ready to fund us ten times more than it offered initially as a token of commendation for our efficient fight against this virus. The World Bank has even asked the Healthcare Ministry to share the experience. Meanwhile, the IMF continues to demand from us quarantine measures, isolation, a curfew. This is nonsense. We will not dance to anyone’s tune,” said the president.
A healthcare firm which employs the prominent Conservative politician Owen Paterson as a paid consultant has been awarded a £133m contract without any other firms being given the opportunity to bid for the work.
The Department of Health and Social Care (DHSC) has given Randox the contract to produce testing kits to help respond to the coronavirus pandemic. It was awarded “without prior publication of a call for competition”, according to details of the contract seen by the Guardian.
Letter dated 17 March 2020 to Chief executives of all NHS trusts and foundation trusts.
ANNEX: CORONAVIRUS COST REIMBURSEMENT This guidance sets out the amended financial arrangements for the NHS for the period between 1 April and 31 July. These changes will enable the NHS and partner organisations (including Local Authorities and the Independent Sector) to respond to COVID-19. We will continue to revise this guidance to reflect operational changes and feedback from the service as the response develops.
We will shortly be making a payment on account to all acute and ambulance providers to cover the costs of COVID-19-related work done so far this year, with final costs for the current financial year being confirmed as part of the year end processes. This initial payment will be based on information already submitted by providers. Future payments will be based on further cost submissions.
All NHS providers and commissioners must carefully record the costs incurred in responding to the outbreak and will be required to report actual costs incurred on a monthly basis. Accurate record keeping during this time is crucial – record keeping must meet the requirements of external audit, and public and Parliamentary scrutiny.
To support reimbursement and track expenditure we will in due course be asking all relevant organisations to provide best estimates of expected costs from now until the expected end of the peak outbreak. We will provide further guidance with relevant assumptions in order to support you in making these estimates.
Dr. Wodarg is reassuring for anyone concerned about ‘the virus’. That danger is no greater than in any other flu season (now also based on tens of international leading scientists analyzing actual figures from all over the world). Wodarg’s message is disturbing when you wonder how the whole world can be fooled by such a clearly fact-free ‘panic’ allowing itself to be led to the curtailment of the most fundamental freedoms. A world that thinks it has to prepare itself for a ‘new normal’. In which incredibly dangerous and extremely undesirable ’solutions’ such as ‘mass vaccination’, ‘contact tracing’, and other ‘surveillance’ are seen as attractive.
https://youtu.be/BrBuv6kq6Rc
Topics discussed:
Coronaviruses are very common so no-one was interested in them until recently as they’re well studies. COVID-19 ‘is not very special’.
China ‘solved’ its epidemic by stopping tests.
Why Italy had a high death rate.
The effect of hydroxychloroquine on people with certain genetic deficiencies.
Conflicts of interests and financial incentives for testing.
We never get herd immunity from coronaviruses.
We don’t need herd immunity for coronaviruses. They will ‘hitchhike’ for a period of time and then switch hosts species.
It’s very difficult to quarantine people for respiratory viruses; the COVID-19 had already spread so the lockdown was nonsense.
The historical data does not show COVID-19 being a severe disease.
EuroMOMO data is not transparent. Dr. Wodarg has become very skeptical about the EuroMOMO statistics.
If we are observing the virus, there should be no difference between the countries’ charts. (Mathematician Andrew Mather has made similar observations in his videos.)
There are so many factors that affect mortality rates but there is no serious discussion.
Perhaps people are being killed by experimental treatment. WHO show 1,200 trials worldwide for clinical trials. There may be irregularities.
Possible attempt to use deaths Africa to spread more fear.
Observational studies as a way to bribe doctors and market drugs.
The side-effects of drugs used in Italy and Spain.
Watch what will happen in Africa.
The reaction to COVID-19 is politics and has nothing to do with medicine.
Raising the possibility of immunity passports.
German health minister is a lobbyist for the pharmaceutical industry.
Data from contact tracing apps is ‘gold’ for the pharmaceutical industry.
The influence of Bill & Melinda Gates foundation and the WHO in the negotiation in vaccine contracts. Only Polish Minister for Health resisted.
Don’t accept the RNA vaccine, which is a new method and has been developed in a very short time. There is no experience with RNA vaccine for infectious diseases.
‘Bill Gates is crazy.’ How can someone promote the vaccination of the planet with a vaccine developed in 1 1/2 years. It has not even been controlled for cancer. You need at least 5 years to see if a cancer grows. If you change RNA, you don’t know.
RNA vaccines require very thorough clinical studies over a long period of time. There are many complications to consider.
Politicians always strive for power. We as a people have to show them how they get power and how they lose it.
In the years following the [Swine Flu] pandemic, the World Health Organisation (WHO) faced fierce criticism over its handling of the situation.
Some medical experts doubted whether the H1N1 outbreak was really a pandemic at all.
Dr Wolfgang Wodarg, a German doctor and former member of parliament, had been watching the spread of swine flu in Mexico City – where the virus was first recorded – and was puzzled at the reaction of the WHO.
Dr Wodarg eventually launched an inquiry into the Swine Flu pandemic and the WHO’s dealings with the pharmaceutical industry in the lead up to the N1H1 pandemic.
Traffic log cookies are used to measure site traffic. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.