There is uncertainty about the effects of face masks. The low to moderate certainty of evidence means our confidence in the effect estimate is limited, and that the true effect may be different from the observed estimate of the effect. The pooled results of RCTs did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks. There were no clear differences between the use of medical/surgical masks compared with N95/P2 respirators in healthcare workers when used in routine care to reduce respiratory viral infection. Hand hygiene is likely to modestly reduce the burden of respiratory illness, and although this effect was also present when ILI and laboratory‐confirmed influenza were analysed separately, it was not found to be a significant difference for the latter two outcomes. Harms associated with physical interventions were under‐investigated.
Norway
Browse the articles related to this topic below.
Join our community on Guilded.
Norway, Sweden and Iceland had the lowest relative cumulative excess mortality.
- Between the week ending 3 January 2020 (week 1 2020) and the week ending 1 July 2022 (week 26 2022), the UK’s relative cumulative excess mortality was 3.1% above the average of 2015 to 2019; this was over a third less than the cumulative excess mortality in the week ending 18 June 2021 (week 24 2021; the period of the previous article), at 5.8%.
- The UK had the 16th highest relative cumulative excess mortality of the 33 countries analysed (UK, its constituent countries, and 28 European countries), and 15th highest of 28 countries when constituent countries are removed.
- The majority of European countries analysed (25 of 33) experienced above average relative cumulative excess mortality for the whole period, with eight countries showing relative cumulative mortality below average.
- Bulgaria had the highest relative cumulative excess mortality at 18.2% above average, followed by Poland (13.3% above average) and Romania (12.2% above average); Norway had the lowest with 4.1% below average, followed by Sweden (4.0% below average) and Iceland (3.9% below average).
- The majority of European countries (22 of 33) had higher relative cumulative excess mortality in those aged 65 years and over compared with those aged under 65 years.
- The UK had the fifth highest relative cumulative excess mortality rate in those aged under 65 years (8.3% above average); in those aged 65 years and over in the UK, the cumulative excess mortality rate was the 19th highest (2.2% above average).
- Overall, 19 of the 33 European countries had a decrease in their relative cumulative excess mortality rates since the last release (week ending 18 June 2021), including the UK and constituent countries; the largest decrease was in Czechia (5.4 percentage points lower), whereas the largest increase was in Cyprus (5.4 percentage points higher).
The risk of myocarditis in this large cohort study was highest in young males after the second SARS-CoV-2 vaccine dose, and this risk should be balanced against the benefits of protecting against severe COVID-19 disease.
https://jamanetwork.com/journals/jamacardiology/fullarticle/2791253
Archive link: https://web.archive.org/web/20230000000000*/https://jamanetwork.com/journals/jamacardiology/fullarticle/2791253
Iceland on Friday suspended the Moderna anti-COVID vaccine, citing the slight increased risks of cardiac inflammation, going further than its Nordic neighbours which simply limited use of the jabs.
…This decision owed to “the increased incidence of myocarditis and pericarditis after vaccination with the Moderna vaccine, as well as with vaccination using Pfizer/BioNTech,” the chief epidemiologist said in a statement.
https://medicalxpress.com/news/2021-10-iceland-halts-moderna-jabs-heart-inflammation.html
Here is statement from Dr. Malcolm Kendrick which deserves to be archived in full. Links to the to original post and archive can be found below.
Thank you to the many people who have e-mailed me recently and asked if I have been silenced. I have not. I have had letters from Public Health England and the General Medical Council, informing me that I was under investigation for daring to question anything about COVID19, particularly vaccines.
The good news is the investigations ended up nowhere, and were closed down. I have also had irate phone calls from doctors, telling me that I must not question vaccination and suchlike. This has been somewhat wearing and has caused me to remain silent for a while and think about things.
However, I do know how to play the medical regulations game. Don’t make a statement you cannot reference from a peer-reviewed journal. Don’t give direct advice to people over the internet. Provide facts, and do not make statements such as ‘vaccines are killing thousands of people.’ Or suchlike.
Not that I ever would. My self-appointed role within the COVID19 mayhem, was to search for the truth – as far as it could be found – and to attempt to provide useful information for those who wish to read my blog.
The main reason for prolonged silence, and introspection, is that I am not sure I can find the truth. I do not know if it can be found anymore. Today I am unsure what represents a fact, and what has simply been made up. A sad and scary state of affairs.
This is not just true of the mainstream and the mainstream media, which has simply decided to parrot all Government and WHO statements without any critical engagement…or thought. For example, the BBC intones that ‘In the last day, fifty people died within twenty-eight days of a positive COVID19 test…’ Or a hundred, or six. What the hell is this supposed to mean? It means nothing, it is the very definition of scientific meaninglessness.
Especially when it seems that very nearly a half of those admitted to hospital with COVID19 were not admitted to hospital with COVID19. They were admitted with something else entirely, then had a positive test whilst in hospital. In short, they were not admitted to hospital with COVID19, and almost certainly did not die of COVID19. They died with a positive COVID19 test. With, not of.
But the misinformation is equally a problem for those on the other side. Claims are made for the benefits of Ivermectin and hydroxychloroquine that simply do not stand up to scrutiny. Yes, I believe both drugs may provide some benefit, but not the claimed 90% reduction in deaths that I have seen trumpeted.
So, I have given up on COVID19. It is a complete mess, and I feel that, without being certain of the ground under my feet, I have nothing to contribute. I too am in danger of starting to make statements that are not true.
However, before leaving the area entirely, I would like to make clear some of the things I currently believe to be true, and what I do not believe to be true. If this is of any assistance to anyone. Very little is referenced, because I can very easily find a contradictory reference to any reference I provide. For each fact, there is an equal and opposite fact.
1: SARS-CoV2 exists
Many people have stated, probably correctly, that the SARS-CoV2 virus has never been fully isolated. Whatever exactly that means. Have Koch’s postulates been met? [see a bit later on] I think for viruses, Koch’s postulates are very rarely, if ever, met. Does it matter, not really.
Despite this gap I believe that SARS-CoV2 truly is a ‘new’ virus that did not exist before. So, it must have mutated somewhere, or been mutated somewhere, from another coronavirus… probably. Although it seems that SARS-CoV2 does not mutate. Instead, it creates variants which, somehow or other, is a completely different process to a mutation! I have found that language in this area means little, and words are simply twisted to suit a particular narrative.
I feel it is most likely this mutation occurred within a laboratory in Wuhan during gain of function research. But I don’t suppose we will ever know. It seems unlikely to be something that the Chinese authorities are ever going to admit… ever. As a general rule, the more fervently, and angrily, the Chinese state denies something – the more likely it is to be true.
This is a special case of a general rule that I modestly call the ‘Kendrick reverse meaning law.’ Which developed from P.G. Wodehouse’s observation that ‘When an Englishman says ‘trust me’ it is time to start counting the spoons.’
This reverse meaning was seen clearly when Matt Hancock (UK Health Secretary at the time) stated that ‘Right from the start we’ve tried to throw a ring of steel around our care homes.’ Which actually meant that ‘Right from the start we threw care homes under a bus.’ Unless, what he actually meant was that the ring of steel was put up to stop care home residents escaping. ‘Halt, who goes there….’ Sound of heavy machine gun fire, whistles screeching, attack dogs baying at the leash. ‘Go for the Zimmer frames, that should bring them down.’
2: SARS-CoV2 is generally more deadly than influenza
Of course, SARS-CoV2 is most certainly not deadlier than the influenza epidemic of 1918-19. Which is estimated to have wiped out 2% of the entire world’s population. It is probably not more deadly than the 1957 epidemic, or the 1967 influenza epidemic. But it seems more deadly than anything in the last forty years, or so. So, a bit more deadly than most influenzas that sweep through humanity every year, or so. Give or take.
Currently, SARS-CoV2 is reckoned to have killed four and half million people across the Globe. Which is 0.07% of the world’s population. However, there is an immediate problem here. With influenza, we count for one year, then start again the next year. With COVID19 we have just kept on counting, adding this year figures to last years, and so on!
Eventually, therefore, assuming COVID19 comes and goes like the flu, and we just keep on counting without end, it will end up killing a hundred million. Making it the deadliest virus ever. Far worse than any influenza? At the current rate this will take another thirty years, or so. Within one thousand six hundred and sixty-six years it will have killed everyone. Of course, there will have been a few billion replacement humans created during that time.
What is far more important is to know the infection fatality rate (IFR)? That is, what percentage of those infected with SARS-CoV2 will die? This, I am afraid, we are never going to know, as the definition of what the word ‘infected’ means has flipped this way and that and can never be pinned down.
Does it mean a positive test? Does it mean a positive test plus symptoms? [Which used to be called a ‘case’] Does it mean something else. What does infected actually mean…
Here, I defer to the Master – Lewis Carroll:
‘When I use a word,” Humpty Dumpty said in rather a scornful tone, “it means just what I choose it to mean — neither more nor less.”
“The question is,” said Alice, “whether you can make words mean so many different things.”
“The question is,” said Humpty Dumpty, “which is to be master – – that’s all.”
Accepting that no-one will define what COVID19 infection actually means, I believe the infection fatality rate is, (using previous used definitions) settling at around 0.15%. At least it was last time I looked. This was never enough to justify the panicked actions that have taken place around the globe. Never.
3: The figures make no sense – and never will
One of the central problems here, form which all other problems flow, is that the PCR (polymerase chain reaction) test is the test against which the PCR test itself is tested. We have nothing better. So, we are completely reliant on it being accurate. However, we cannot know how accurate it truly is, because there is no test against which to compare it.
I mentioned Koch’s postulates earlier. These are the tests which can prove if a ‘micro-organism’ is actually causing the disease. The ultimate gold standard:
The microorganism must be found in abundance in all organisms suffering from the disease, but should not be found in healthy organisms. The microorganism must be isolated from a diseased organism and grown in pure culture. The cultured microorganism should cause disease when introduced into a healthy organism. The microorganism must be re-isolated from the inoculated, diseased experimental host and identified as being identical to the original specific causative agent. And good luck with all of that. The truth is that these postulates can work for bacteria, but not really for viruses. Because it is very difficult to meet them. I am not sure if they have ever been truly met for any virus.
On the matter of finding out if the virus is truly present, in anyone diagnosed with COVID19, here is a letter that was published in the BMJ in October last year
‘We are told that the virus is everywhere – in the air, in our breath, on fomites, trapped in masks – yet public health authorities seem not to be in possession of any cultivable clinical samples of the offending pathogen.
In March 2020, the World Health Organisation instructed authorities not to look for a virus but to rely instead on a genome test, the RT-PCR, which is not specific for SARS-CoV-2 (1) (2).
A Freedom of Information request to Public Health England about cultivable clinical samples or direct evidence of viral isolation has no information and refers to the proxy RT-PCR test, quoting Eurosurveillance (3).
Eurosurveillance states: “Virus detection by reverse transcription-PCR (RT-PCR) from respiratory samples is widely used to diagnose and monitor SARS-CoV-2 infection and, increasingly, to infer infectivity of an individual. However, RT-PCR does not distinguish between infectious and non-infectious virus. Propagating virus from clinical samples confirms the presence of infectious virus but is not widely available (and) requires biosafety level 3 facilities” (4).
The CDC admits that, “no quantified virus isolates of the 2019-nCoV are currently available”, and used a genetically modified human lung alveolar adenocarcinoma cell culture to, “mimic clinical specimen”(5).
It appears, therefore, that we have public health bodies without clinical samples, a test which is non-specific and does not distinguish between infectivity and non-infectivity, a requirement for biosafety level 3 facilities to even look for a virus, yet we are led to believe that it is up all our noses.
So, where is the virus?’
(1) https://www.who.int/publications/i/item/10665-331501
(2) https://www.bmj.com/content/369/bmj.m2420/rr-5
(3) https://www.whatdotheyknow.com/request/679566/response/1625332/attach/ht…
(4) https://www.eurosurveillance.org/content/10.2807/1560-7917.ES.2020.25.32…
(5) https://www.fda.gov/media/134922/download 1
After reading this, do I still think SARS-CoV2 exists? Yes, I do. I firmly believe that I watched people dying of it, from it. They died in a way I have never seen people do so before, and I have seen a lot of people die. They seemed quite well, then suddenly their oxygen sats dropped like a stone – they still seemed okay otherwise – then they died. The end.
Very strange, and rather disturbing. I started slipping an oxygen saturation monitor onto my finger from time to time. Just in case. 99% is my average reading, if you are interested. It never dropped.
However, getting back to the testing. If you truly want to confirm the presence of a virus in a sample, you need to send it to biosafety level 3 facilities to isolate it, grow it (not really the correct word for a virus), and suchlike. This is never done in the clinical setting.
You could argue that if you wait for antibodies to develop, you can ‘prove’ that someone was infected, or not, and thus work out how accurate the PCR test has been retrospectively. Perhaps…
I speak as someone who needed seven Hepatitis B vaccinations before I produced any detectable antibodies. Did I have immunity after the first six, or not? Am I someone who simply does not make many antibodies, but still have immunity through other mechanisms? Do others simply not produce antibodies, or their level drops so fast, that they effectively disappear?
Yes, serological testing (looking for antibodies), has its own very significant problems.
‘Serological tests for SARS-CoV-2 have accuracy issues that warrant attention. They measure specific antibody responses which may take some weeks to develop after disease onset reducing the sensitivity of the assay. If blood samples were collected during the early stage of the infection, they may produce false negative results. They do not directly detect the presence of the virus. Further, antibodies may be present when SARS-CoV-2 is no longer present giving false positive case diagnosis.’ 2
In reality, we are relying on a PCR test to diagnose SARS-CoV2 infection, the accuracy of which is entirely dependent on believing that the test is accurate. Yes, that is the route to madness.
At present, in the UK, we are doing about one million tests a day 3.
We are getting about thirty thousand ‘positive’ results. Or, about 3% positive. How many of these are truly positive? Well, you can take a wild guess on that one. At one point, the CDC stated that 30% of the PCR tests were false positives. A ‘false positive’ means that test says you have the disease, when you do not. [A false negative informs you that you do not have the disease, when you do] 4.
The thirty per cent cannot be the case currently, because that would mean if you did one million tests, you would get more than three hundred thousand false positives. Instead we are getting thirty thousand, which means that it is impossible for the false positive rate to be higher than three per cent.
So, what is the true rate? Well, if is three percent, then virtually every single positive test is a false positive test. [Three per cent of one million is thirty thousand] Which would mean that no-one in the UK currently has COVID19, and everything we are doing is completely pointless. It also means that people admitted to hospital with COVID19 do not have the disease, they are suffering from, and dying from, something else with a false positive COVID19 false test stamped on their forehead.
Is it possible that no-one actually is infected with SARS-CoV2? Well, it is certainly not impossible. Here is a graph of overall mortality (risk of dying of anything) from England. These figures, unlike most others, are pretty much fully reliable. Someone is either dead, or they are not. It is a difficult thing to get wrong, or manipulate. There can be some delay in registering a death, but this is not normally a major issue.
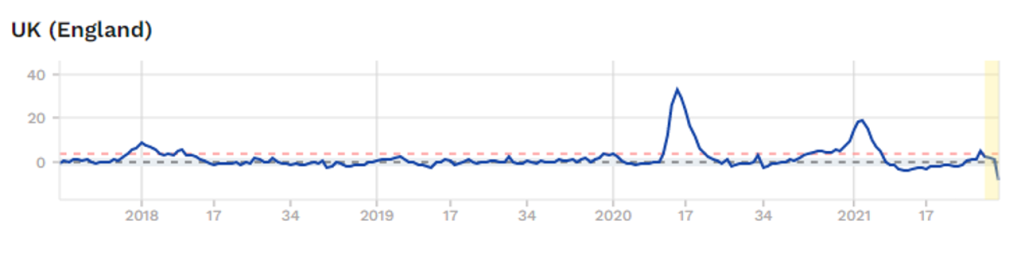
The graph starts in last quarter 2017. As you can see, a spike in overall mortality in Spring 2020, A spike in Winter 2020/21. Currently, no excess mortality at all. So, if COVID19 is infecting hundreds of thousands of people each week, it is not showing up as any excess deaths… at all 5.
Does this mean that COVID19 has gone, and we are rushing around panicking about false positive tests? Or is it still here? Still here I think… but who knows… who knows.
This is the main reason I have given up. I just don’t know what to believe – apart from overall mortality figures. The figures are spun and massage, twisted and mangled.
Another reason why I have given up trying to make any sense of COVID19 is the enormous differences in overall mortality seen in countries that are virtually identical in life expectancy, healthcare systems, actions taken against COVID19 etc. etc.
Afters studying the figures from England, I looked at the figures from Northern Ireland.
Both countries [yes, Northern Ireland is not actually a separate country, it is part of the UK] did almost exactly the same things when it came to COVID19. They both have the National Health Service, they are as close to each other as can be – in terms of COVID19, and most other things. Here is the graph of overall morality for Northern Ireland.
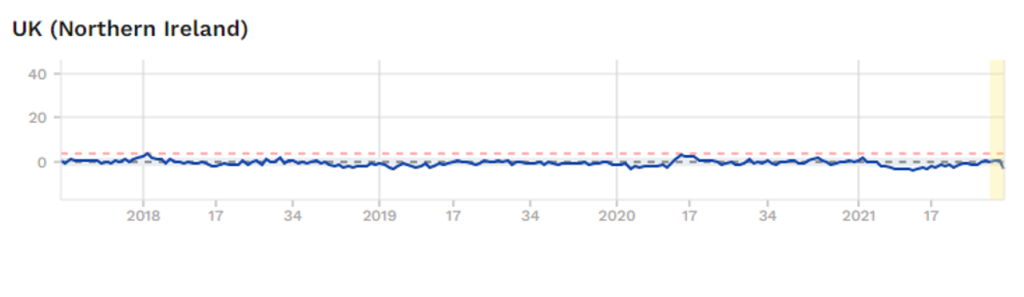
Which means that something very dramatic happened in England, with regard to COVID19? Yet nothing happened in Northern Ireland. This, to me, is fascinating, although I cannot explain it. However, I know that if you were able explain why these two graphs are so weirdly different, you will be unearthing some critical truths with regard to COVID19.
Of course, no-one is remotely interested in such anomalies. Instead, they point to a country like Norway and say – ‘Look how well they did with their rapid lockdown, and preventing people crossing the border’. No-one points to Northern Ireland and says, ‘look how well they did with all their….’ All their what? All their doing exactly the same as England.
Yes, Northern Ireland does not fit with the approved narrative, so it is ignored. Anything that does not fit with the mask wearing, social isolating, vaccination will save the world narrative is simply ignored.
Or it is shouted down or censored by the self-appointed Fact-checkers. Those mighty intellects who can determine what is true, and what is not. It was thoughtful of them to descend from Mount Olympus to mingle amongst feeble minded humanity and tell us what we should, and should not, be thinking. We must all be eternally grateful that the ‘Truth Gods’ now live amongst us, to firmly inform us all what, and how, we should be thinking. And shut us down if we veer from the official narrative.
Anyway, faced with a situation where there are almost no facts that can be relied upon, from anywhere, I have officially removed myself from all discussions on the matter of COVID19.
Instead, I shall return to other areas where, whilst the truth is constantly battered and bruised, and lying in a bruised heap the corner, it is still breathing … just about alive. Sometimes it is capable of weakly raising its head and whispering quietly into my ear. I shall let you know what it says.
1: https://www.bmj.com/content/370/bmj.m3379/rr-2
2: https://systematicreviewsjournal.biomedcentral.com/articles/10.1186/s13643-021-01689-3
3: https://coronavirus.data.gov.uk/?_ga=2.38943459.111756282.1590603430-1775824629.1590603430
4: https://www.bmj.com/content/373/bmj.n1411/rr
5: https://www.euromomo.eu/graphs-and-maps/
https://drmalcolmkendrick.org/2021/09/03/i-have-not-been-silenced/
At least three claims over serious side effects of Oxford-made vaccine AstraZeneca have been upheld in Norway, resulting in financial compensation. Dozens more are expecting a ruling in connection with coronavirus-jab reactions.
The Norwegian System of Patient Injury Compensation (NPE) will make payments to three applicants badly affected by the Oxford-AstraZeneca vaccine, it announced on Friday. It officially confirmed that the vaccine, currently suspended in the European country, has resulted in severe cases of blood clots and low platelet counts in these patients, one of whom died.
https://www.rt.com/news/528174-norway-astrazeneca-vaccine-compensations/
Manufacturers have been granted exemption from liability for any resulting harm. Ruud Dobber, a member of AstraZeneca’s senior executive team, said: “This is a unique situation where we as a company simply cannot take the risk if in … four years the vaccine is showing side effects.” (The government has taken on the liability and has an insurance scheme in place.)
https://www.thetimes.co.uk/article/why-not-giving-children-covid-vaccine-lw5kpn5m5
Categories
So what about Sweden, huh? – The Spectator
It’s amazing how often Sweden still crops up in conversations. It didn’t impose tough lockdown, kept primary schools and core economic activities functioning, issued clear guidelines and relied on voluntary social distancing and personal hygiene practices to manage the crisis. For harsh lockdowns to be justified elsewhere, Sweden had to be discredited. Hence the harsh criticisms of Sweden’s approach last year by the New York Times, Newsweek, USA Today, CBS News and others.
But with Sweden’s demonstrable success, goalposts have shifted. Every time it’s mentioned as a counter to Europe’s high Covid-toll lockdown countries, the response now is: ‘But their Nordic neighbours did much better. Look at Denmark’. Let’s ‘interrogate’ this argument.
Meanwhile, the disconnect between what ordinary people can see with their own eyes and the Covid regulations only confirms the idea that Government pronouncements are no longer to be taken literally. The rules are starting to seem symbolic and removed, subject to broad reinterpretation. While the polling shows that people are content with the official pace of reopening, the mobility data (what people are actually doing) shows they have been quietly reopening their lives since January. Apple data now shows use of public transport in London up to nearly 70 per cent of normal from nearer 30 per cent at the start of this lockdown.
https://www.telegraph.co.uk/news/2021/04/15/covid-no10-treating-public-like-fools/
The European nation reported that 23 elderly people have died within days of taking the Pfizer COVID-19 vaccine, with 13 of those deaths said to be related to “side effects”. All those who suffered supposed side effects were nursing home patients and at least 80 years old.
Categories
Prof. Carl Heneghan On Masks
- Masks and gloves have been shown in studies to help in the medical setting but not in the home setting.
- Cloth masks are worse and may increase infection.
- Masks in the UK were supposed to reduce infections by 40% but in fact, infections went up.
- Study in Norway: 200,000 people would have to wear a mask in order to prevent one infection. Public health impact of mask wearing is negligible.
- This advocating mask-wearing have cherry-picked low-quality observational evidence to suit the evidence.
Carl Heneghan is a clinical epidemiologist with expertise in evidence-based medicine, research methods, and evidence synthesis.
He is Director of the NIHR SPCR Evidence Synthesis Working Group a collaboration of nine primary care departments across UK universities. He set up and directs the Oxford COVID Evidence Service, has over 400 peer-reviewed publications (current H Index 67); published 95 systematic reviews. He is Editor in Chief of BMJ Evidence-Based Medicine, and Editor of the Catalogue of Bias.
Director of CEBM & Programs in EBHC
Editor in Chief, BMJ EBM
NHS Urgent Care GP
NIHR Senior Investigator