The difference between what the government was telling us and what their information was telling us was so extreme and outrageous.
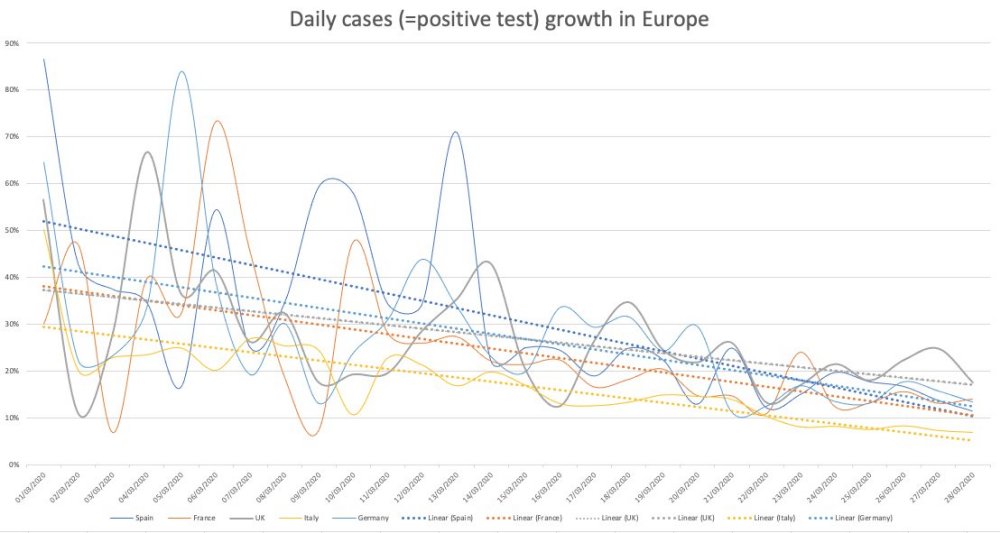
Exponential means a “constant rate of growth.” The government data in March was clearly showing that the COVID-19 was declining, not growing exponentially. This was the same in all countries you could see the data. [See chart 1]
A constantly declining growth rate will make a bell curve. The government were standing in front of bell curve graphs during their briefings yet they were telling us we were in the middle of the epidemic.
It was very clear that we were heading to a peak sometime around early to mid-April.
You don’t have to be complicated mathematics to see that COVID-19 was running out of steam almost from day one.
The conclusion from the Centre for Evidence-Based Medicine seems to be that it’s impossible to predict if there will be a second wave.
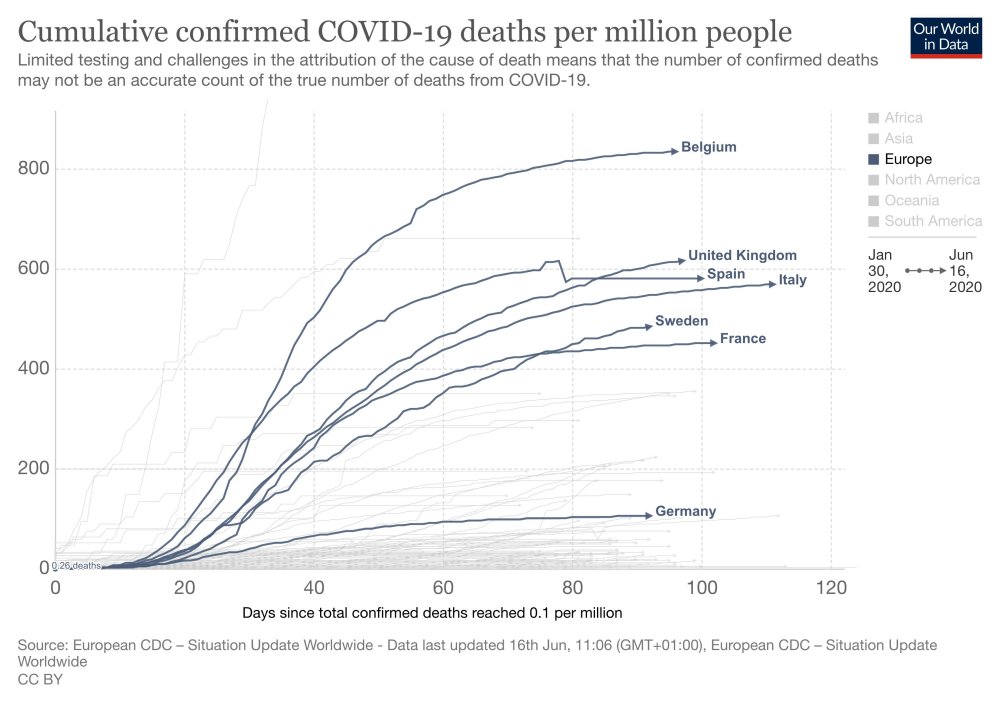
Sweden’s epidemic looks identical to the UK’s but they did not lockdown. Their datapoint indicates there won’t be a second wave. There has been no spike in Denmark either. [See chart 2]
Unknowns: has summer affected COVID-19 and will there be a mutation?
Will illnesses during the autumn and winter be mis-attributed to COVID-19? Poor media coverage means that we can’t be sure.
Symptoms of COVID-19 are very similar to the flu. Something could look like a second wave but will we really know?
The lockdown is costing a Brexit bill a week.
The government response seems to have been skewed by Neil Ferguson’s modelling data. The make-up of government advisors seems to be a recipe for groupthink, which is very dangerous.
Epidemiology (the way a disease spreads through the population) is not complicated science. The government could have had lots of people who were very good at this but they didn’t.
We should have cocooned the vulnerable, make sure the NHS has capacity and “let it rip” through the population.
We should never have had an open-ended lockdown.
The ‘R number’ is just the difference of in the number of people infected after each generation of a disease. Britain crossed the ‘magical R of 1’ line a few days before lockdown and the same day as Sweden. Whatever interventions have been done doesn’t seem to have had any effect. [See chart 3]
COVID-19 is mostly a care home and hospital disease. This was obvious very early on. Old people should not have been moved from hospitals into care homes. It seems as if we knowingly seeded the most vulnerable environment with the disease.
37% of our deaths are care home residents but they are only 0.5% of our population. Of them are dementia sufferers.
Over 20% of the infections were picked up in the hospitals. COVID-19 seems more like MRSA than influenza in that it’s an infection control problem.
COVID-19 is much more comparable to flu for the rest of the population.
1968 flu killed 80,000 people in the UK.
This last winter was a low flu winter. It’s quite possible that the people who died of COVID-19 are those who didn’t die.
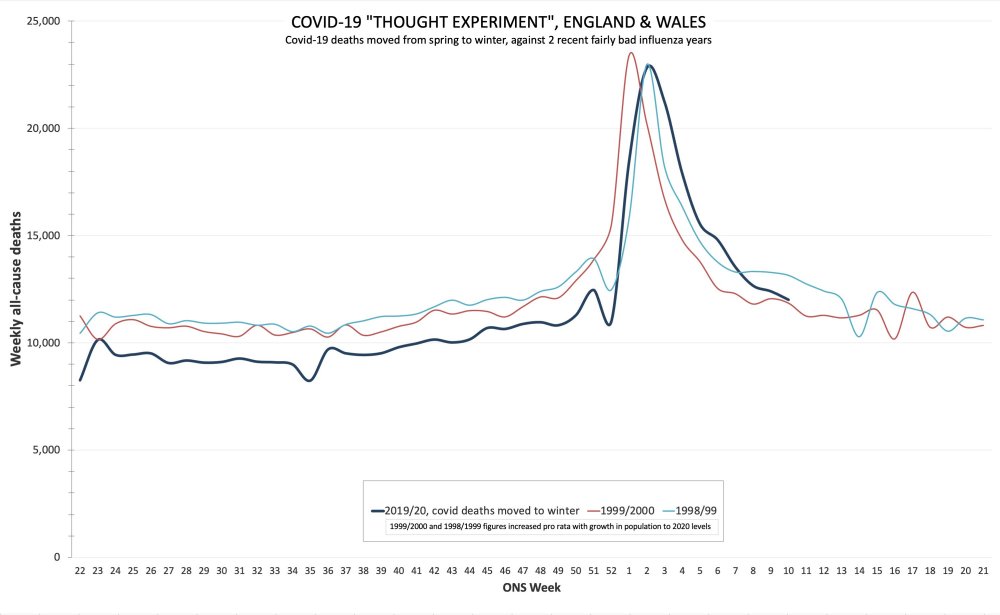
If you overlay COVID-19 deaths with the 2000 flu season, they look very similar. [See chart 4]
95% of deaths have had another serious disease. Most people have almost no chance of dying from COVID-19.
If you are under 40, you have more chance of being struck by lightning that dying of COVID-19.
If you are under 60, you have more chance of drowning.
At any age, you have more chance of dying on the roads than dying of COVID-19.
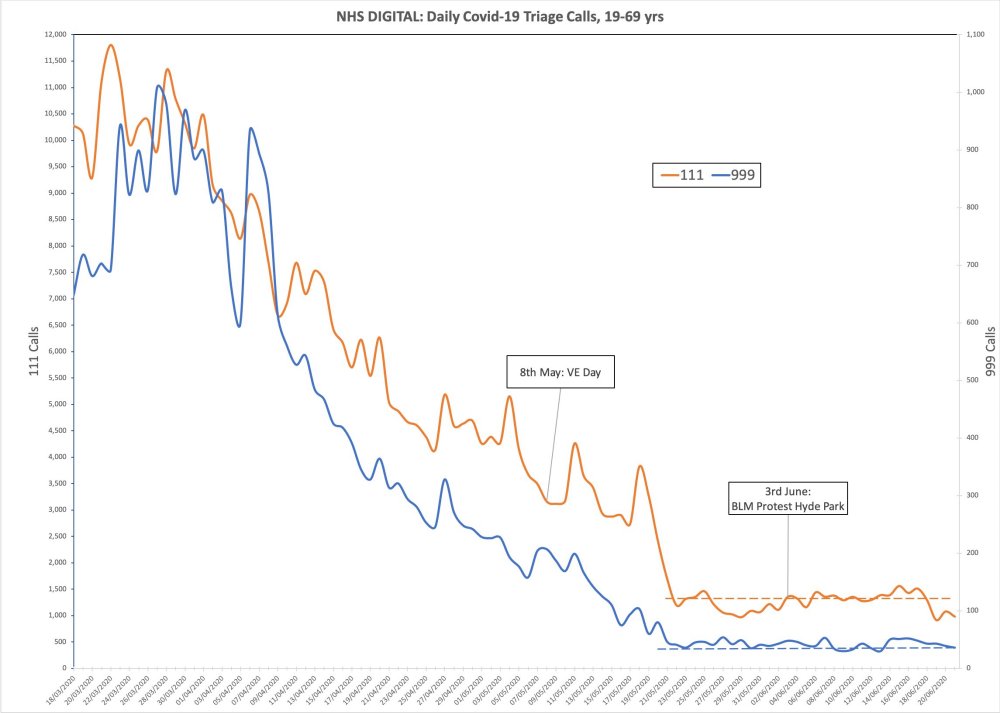
Lead indicators of 111 and 999 calls with COVID-19 symptoms show there was no spike after VE Day celebrations or BLM protests. In fact, it was even coming down at lockdown. That lockdown was big change for COVID-19 is invisible in the data. [See chart 5]
Charts
Chart 1: COVID-19 was declining in Europe as of march. It was not growing exponentially
Chart 2: Sweden’s epidemic looks similar to the UK’s but they did not lock down.
Sweden has had fewer covid deaths per capita than Belgium, Spain, Italy or the UK, and its children <16 have missed no school. @AlistairHaimes, 17 June 2020
Chart 3: Britain crossed the ‘magical R of 1’ line a few days before lockdown
UK Rt (“R number”), late Feb to early April. Lockdown did the square root of nothing. Hand-washing advice early March does look to have caused a massive drop in R, as you’d expect. @AlistairHaimes, 5 May 2020
Chart 4: COVID-19 deaths overlayed with the 2000 flu season
If covid deaths had happened in winter rather than spring. Shown against two recent moderately bad influenza years, for comparison. @AlistairHaimes, 23 June 2020
There were 3 influenza pandemics in the 20th century, and there has been 1 so far in the 21st century. Local, national, and international health authorities regularly update their plans for mitigating the next influenza pandemic in light of the latest available evidence on the effectiveness of various control measures in reducing transmission. Here, we review the evidence base on the effectiveness of nonpharmaceutical personal protective measures and environmental hygiene measures in nonhealthcare settings and discuss their potential inclusion in pandemic plans. Although mechanistic studies support the potential effect of hand hygiene or face masks, evidence from 14 randomized controlled trials of these measures did not support a substantial effect on transmission of laboratory-confirmed influenza. We similarly found limited evidence on the effectiveness of improved hygiene and environmental cleaning. We identified several major knowledge gaps requiring further research, most fundamentally an improved characterization of the modes of person-to-person transmission.
Researchers found school closures had little effect on preventing coronavirus transmission compared to that of the flu.
Under-20s are half as likely to catch COVID-19 as over-20s, making school closures less effective at stopping the spread of the virus, a new scientific study has found.
Researchers at the London School of Hygiene and Tropical Medicine found that susceptibility to the coronavirus was low for younger people, before increasing around the age of 20.
On average, roughly 20% of the unvaccinated had serologic evidence of influenza infection, but up to three quarters of the infected were asymptomatic. The proportions did not vary significantly between seasonal and pandemic influenzas. The pandemic H1N1 strain was associated with less severe symptoms than the seasonal H3N2 strain.
Note: The video has been removed from Vimeo but has been archived on BitChute (see embedded below highlights).
James talks with Professor Dolores Cahill, a world renowned immunologist who has advised the Irish government and the EU.
We should end the lockdown. Quarantining healthy people was a huge mistake, should never have been done and should never happen again.
All the available information tells us there’s no longer any basis for the lockdowns. The economic harm and resulting health effects could be five times higher than those caused by the virus. The adverse health implications of poverty is well-known and has lots of supporting data.
The immunology community knew in January and February that there was nothing very special about COVID-19.
There are lots of clinical trials showing the usefulness of vitamins C, D and Zinc for preventing symptoms of corona-type viruses.
It is also very well established that hydroxychloroquine, which is a very safe drug, can be used as a treatment.
There was no need to ramp up the hospital care system because there were established methods for prevention and treatment.
It was known that the virus would circulate the world in a month. Professor Cahill was surprised at the lockdown because the ‘virus was gone.’ There is clearly enough data for this.
COVID-19 (also known as SARS-CoV-2) is about 80% the same as SARS-CoV-1 in 2003. These types of viruses last about 6 weeks in each location before naturally ‘dying off’ as people become exposed and then developing immunity.
80 out of 100 people would have developed antibodies within 10-11 days and become immune for life without experiencing symptoms.
Although COVID-19 is a novel virus, it can be ‘recognized’ by the immune system of anyone who had already been exposed to SARS-CoV-1. This is because of COVID-19’s 80% similarity to the earlier 2003 virus.
With these types of viruses, you will be negative for the PCR test (which tests for the presence of the virus) after recovery but you will test positive for the antibodies.
You don’t need the lockdown if you boost your immune system. in fact, the lockdown made matters worse by depressing people’s immune system. Sunshine, interacting with people, shaking hands–all these help to boost your immune system.
Elderly people should be taking vitamin C, D and Zinc to protect their immune systems. People with underlying conditions, or those who develop symptoms, should contact their doctor to consider prescribing off-label hydroxychloroquine.
Symptoms: flu-like for the first five days. If it gets worse and you develop a cough, that’s when you need to ring your doctor for treatment. Treatment includes hydroxychloroquine for 3-5 days, with Zinc and AZT antibiotic. This is an established protocol that has been used in many clinical trials in 2020.
There was some reason to be scared of COVID-19 during the very early stages (around January) because because we didn’t know anything about it. However, the media and WHO was fearmongering when they used Wuhan as an example of what would happen everywhere.
From February onward, the immunology community recognized that COVID-19 is the same as a normal virus in most parts of the world. There was something different about Wuhan, Bergamo and New York but t here was no reason to lockdown the rest of the world.
Vaccines have their place and can be safe. However, studies show that animal and human subjects that were given a type of influenza vaccine later reacted badly when they encountered a coronavirus ‘in the wild’. The reaction caused a cytokine storm that either killed the subject or made the subject very ill. The reaction between different types of vaccinated and wild viruses is called viral interference.
People in Wuhan and Bergamo were given a certain type of influenza vaccine. It became apparent around April-May that the high death rates in both cities could be due to viral interference from the administered influenza vaccine.
It has not been possible to make a safe and effective vaccine for the SARS-CoV-1 in 2003. If we have not been able to make a vaccine for this coronavirus, we should not expect a safe vaccine for COVID-19 any time soon. A vaccine developed for COVID-19 would be a complete experiment on those who take it.
The global death rate for COVID-19 is around the same as a bad influenza. Outside of Wuhan, Bergamo and New York, the death rate appears to be less than the normal flu.
Current data shows that the real death rate for COVID-19 is 20 or 30 times less than the initial estimates from the WHO. We now know the death rate is about one in a thousand for the vulnerable and one in five thousand for the healthy. In the under 70s age range, this is lower than the average flu.
It was well-known in February that there was no need for the lockdowns.
There have been no cases of transmission from children.
If we were to end the lockdown, we would need 10 days to prepare. This is because people have not been out and exposed to sunlight. Preparation include taking vitamins C, D and Zinc; getting fresh air; avoiding stress; and making sure doctors have hydroxychloroquine.
It is almost as if the current advice is geared to making sure people get sick in order to support more lockdowns.
There will be no second spike if people take the above precautions to strengthen their immune system.
A recent study shows that people who continued working were healthy. Engaging with other keeps you healthy by strengthening the immune system.
There hasn’t been an open debate in any country about the harm versus benefits of the lockdown. This may be a big reason for why the lockdowns are continuing.
Dr. Rashid A. Buttar and Dr. Judy Mikovits are trying to open the debate about prevention and treatments but their voices are being censored.
The use of hydroxychloroquine as a treatment has been politicized.
Evidence is being cherry-picked in order reach a predetermined goal: a money-making vaccine. The existing prevention and treatment methods don’t make money for big-pharma.
Masks and social distancing is appropriate for something like ebola but not for coronaviruses.
We will build up herd immunity within about two weeks.
We know how COVID-19 is transmitted because it belongs to the family of coronaviruses. It is not transmitted through the air. This has been proven because groups of people in encloses spaces (for example, plane-loads of fruit-pickers) did not all come down with the sickness.
The two meter rule is unnecessary.
There was enough information from many sources for the government and their advisors to know that all these measures are wrong. There should be legal implications for those who advocate continued lockdown. Hundreds of unnecessary deaths should be grounds for a legal tribunal.
There is a high risk of a death spike after lockdown due to other causes, such as cancers, that will attributed to COVID-19. This will be used to support more lockdowns.
The politicians, broadcasters, newspaper editors, ministers for health–everyone complicit in censoring and withholding information from the public about the true nature of COVID-19 needs to be held personally liable for the deaths caused.
Fact #1: The Infection Fatality Rate for COVID-19 is somewhere between 0.07-0.20%, in line with seasonal flu
Fact #2: The risk of dying from COVID-19 is much higher than the average IFR for older people and those with co-morbidities, and much lower than the average IFR for younger healthy people, and nearing zero for children
Fact #3: People infected with COVID-19 who are asymptomatic (which is most people) do NOT spread COVID-19
Fact #4: Emerging science shows no spread of COVID-19 in the community (shopping, restaurants, barbers, etc.)
Fact #5: Published science shows COVID-19 is NOT spread outdoors
Fact #6: Science shows masks are ineffective to halt the spread of COVID-19, and The WHO recommends they should only be worn by healthy people if treating or living with someone with a COVID-19 infection
Fact #7: There’s no science to support the magic of a six-foot barrier
Fact #8: The idea of locking down an entire society had never been done and has no supportable science, only theoretical modeling
Fact #9: The epidemic models of COVID-19 have been disastrously wrong, and both the people and the practice of modeling has a terrible history
Fact #10: The data shows that lockdowns have NOT had an impact on the course of the disease.
Fact #11: Florida locked down late, opened early, and is doing fine, despite predictions of doom
Fact #12: New York’s above average death rate appears to be driven by a fatal policy error combined with aggressive intubations.
Fact #13: Public health officials and disease epidemiologists do NOT consider the other negative societal consequences of lockdowns
Fact #14: There is a predictive model for the viral arc of COVID-19, it’s called Farr’s Law, and it was discovered over 100 years ago
Fact #15: The lockdowns will cause more death and destruction than COVID-19 ever did
Fact #16: All these phased re-openings are utter nonsense with no science to support them, but they will all be declared a success
There were many signs that were really available by the end of February indicating this is a virus that has ‘weak legs.’
The data was all available by the end of February [2020] and anyone who can use Excel could analyse it.
“The best statistical test is the eyeball test.” And if you chart things in Excel, you can very quickly make an instinctive judgement.
No country succeeded in protecting the elderly and nursing homes–it’s hard thing to do.
We had a soft flu season. The people who would have been susceptible to a generic flu were hit by a virus that came late and swept through rapidly. This could explain the high COVID-19 death numbers among the vulnerable.
Many analysts agree that the lockdown did nothing to affect the peak of infections and deaths.
None of the pro-lockdown people seemed to analyse the data and used the data to support lockdown.
Many pro-lockdown scientific colleagues are academics receiving salaries; their lives would not be negatively affected by the lockdown. Scientists love nothing more than staying at home to work.
What really matters is the years lost rather than the number of dead. Life is risky and when you’re old, life is more risky. You’re expecting younger people to give their future to get two more months of life.
While COVID-19 is not the same as the flu, the numbers look very similar.
People rolled over for a lockdown based on no real solid science.
There’s a whole fallacy about the R value because it is dependent on the time you’re infected and no one knows what the time infected is, no one knows about hidden cases.
Injected influenza vaccines probably have a small protective effect against influenza and ILI (moderate-certainty evidence), as 71 people would need to be vaccinated to avoid one influenza case, and 29 would need to be vaccinated to avoid one case of ILI. Vaccination may have little or no appreciable effect on hospitalisations (low-certainty evidence) or number of working days lost.
It is what is known in science as positive feedback or a snowball effect. The government is afraid of its constituents. Therefore, it implements draconian measures. The constituents look at the draconian measures and become even more hysterical. They feed each other and the snowball becomes larger and larger until you reach irrational territory. This is nothing more than a flu epidemic if you care to look at the numbers and the data, but people who are in a state of anxiety are blind. If I were making the decisions, I would try to give people the real numbers. And I would never destroy my country.
Compared to that rise, the draconian measures are of biblical proportions. Hundreds of millions of people are suffering. In developing countries many will die from starvation. In developed countries many will die from unemployment. Unemployment is mortality. More people will die from the measures than from the virus. And the people who die from the measures are the breadwinners. They are younger. Among the people who die from coronavirus, the median age is often higher than the life expectancy of the population. What has been done is not proportionate. But people are afraid. People are brainwashed. They do not listen to the data. And that includes governments.
Any reasonable expert – that is, anyone but Professor Ferguson from Imperial College who would have locked down everybody when we had swine flu – will tell you that lockdown cannot change the final number of infected people. It can only change the rate of infection. And people argue that by changing the rate of infection and ‘flattening the curve’, we prevented the collapse of hospitals. I have shown you the costs of lockdown, but this was the argument in favour of it. But look at Sweden. No lockdown and no collapse of hospitals. The argument for the lockdown collapses.
We randomized 115 children to trivalent inactivated influenza vaccine (TIV) or placebo. Over the following 9 months, TIV recipients had an increased risk of virologically-confirmed non-influenza infections (relative risk: 4.40; 95% confidence interval: 1.31-14.8). Being protected against influenza, TIV recipients may lack temporary non-specific immunity that protected against other respiratory viruses.
In the prepandemic period of our study, we did not observe a statistically significant reduction in confirmed seasonal influenza virus infections in the TIV recipients (Table 3), although serological evidence (Supplementary Appendix) and point estimates of vaccine efficacy based on confirmed infections were consistent with protection of TIV recipients against the seasonal influenza viruses that circulated from January through March 2009 [16]. We identified a statistically significant increased risk of noninfluenza respiratory virus infection among TIV recipients (Table 3), including significant increases in the risk of rhinovirus and coxsackie/echovirus infection, which were most frequently detected in March 2009, immediately after the peak in seasonal influenza activity in February 2009 (Figure 1).
The key findings are that <50% of participants were adherent with mask use and that the intention-to-treat analysis showed no difference between arms. Although our study suggests that community use of face masks is unlikely to be an effective control policy for seasonal respiratory diseases, adherent mask users had a significant reduction in the risk for clinical infection. Another recent study that examined the use of surgical masks and handwashing for the prevention of influenza transmission also found no significant difference between the intervention arms.
Professor Michael Levitt, Stanford Prof. of Biophysics, Cambridge PhD and DSc, 2013 Chemistry Nobel Laureate (complex systems), says that Europe’s COVID19 Excess Deaths plateau at 153,006, 15% more than 17/18 Flu with same age range counts.
Dr. Wodarg is reassuring for anyone concerned about ‘the virus’. That danger is no greater than in any other flu season (now also based on tens of international leading scientists analyzing actual figures from all over the world). Wodarg’s message is disturbing when you wonder how the whole world can be fooled by such a clearly fact-free ‘panic’ allowing itself to be led to the curtailment of the most fundamental freedoms. A world that thinks it has to prepare itself for a ‘new normal’. In which incredibly dangerous and extremely undesirable ’solutions’ such as ‘mass vaccination’, ‘contact tracing’, and other ‘surveillance’ are seen as attractive.
https://youtu.be/BrBuv6kq6Rc
Topics discussed:
Coronaviruses are very common so no-one was interested in them until recently as they’re well studies. COVID-19 ‘is not very special’.
China ‘solved’ its epidemic by stopping tests.
Why Italy had a high death rate.
The effect of hydroxychloroquine on people with certain genetic deficiencies.
Conflicts of interests and financial incentives for testing.
We never get herd immunity from coronaviruses.
We don’t need herd immunity for coronaviruses. They will ‘hitchhike’ for a period of time and then switch hosts species.
It’s very difficult to quarantine people for respiratory viruses; the COVID-19 had already spread so the lockdown was nonsense.
The historical data does not show COVID-19 being a severe disease.
EuroMOMO data is not transparent. Dr. Wodarg has become very skeptical about the EuroMOMO statistics.
If we are observing the virus, there should be no difference between the countries’ charts. (Mathematician Andrew Mather has made similar observations in his videos.)
There are so many factors that affect mortality rates but there is no serious discussion.
Perhaps people are being killed by experimental treatment. WHO show 1,200 trials worldwide for clinical trials. There may be irregularities.
Possible attempt to use deaths Africa to spread more fear.
Observational studies as a way to bribe doctors and market drugs.
The side-effects of drugs used in Italy and Spain.
Watch what will happen in Africa.
The reaction to COVID-19 is politics and has nothing to do with medicine.
Raising the possibility of immunity passports.
German health minister is a lobbyist for the pharmaceutical industry.
Data from contact tracing apps is ‘gold’ for the pharmaceutical industry.
The influence of Bill & Melinda Gates foundation and the WHO in the negotiation in vaccine contracts. Only Polish Minister for Health resisted.
Don’t accept the RNA vaccine, which is a new method and has been developed in a very short time. There is no experience with RNA vaccine for infectious diseases.
‘Bill Gates is crazy.’ How can someone promote the vaccination of the planet with a vaccine developed in 1 1/2 years. It has not even been controlled for cancer. You need at least 5 years to see if a cancer grows. If you change RNA, you don’t know.
RNA vaccines require very thorough clinical studies over a long period of time. There are many complications to consider.
Politicians always strive for power. We as a people have to show them how they get power and how they lose it.
…the report’s assessment is in line with a growing number of international experts who demonstrate that the threat of COVID-19 is no worse than a severe influenza cycle.
Grave errors of judgement in crisis management
Deficits in the regulatory framework for pandemics
Surgical masks and N95 respirators are not effective at preventing the flu. Of the 446 nurses who took part in this study, nearly one in four (24%) in the surgical mask group still got the flu as did 23% of those who wore the N95 respirator.
Influenza infection occurred in 50 nurses (23.6%) in the surgical mask group and in 48 (22.9%) in the N95 respirator group (absolute risk difference, −0.73%; 95% CI, −8.8% to 7.3%; P = .86), the lower confidence limit being inside the noninferiority limit of −9%.
In the interest of public debate, we allow visitors to share opinions, experiences and research that may be of value to others. This is a visitor contribution from our Discussions page.
Bio:Niall McCrae is a senior lecturer in mental health. His research interests are dementia, depression and the impact of social media on younger people’s mental health. He has written three books: ‘The Moon and Madness’ (2011), ‘Echoes from the Corridors’ (with Peter Nolan, 2016) and the forthcoming ‘Moralitis: a Cultural Virus’ (with Robert Oulds, 2020).
Bio:David Kurten is a London Assembly Member. He was elected in 2016 and sits on the Transport, Education, Housing, Fire and Environment committees at London City Hall. Before entering politics he was a Chemistry teacher and taught in schools in the UK, the USA, Botswana, Bermuda and Bosnia-Herzegovina.
Covid-19 and flu vaccination: is there a link?
Niall McCrae & David Kurten
Could the flu vaccine be a factor in deaths from the coronavirus pandemic? Mortality varies widely between countries, some having rates less than ten per million, while western Europe and the USA are in the hundreds. And there is at least a correlation with the extent of flu vaccination in the elderly. The medical establishment tends to cast anyone who doubts the merits of vaccination as an extremist, but we present our case tentatively, and leave it to readers to decide whether this is a reasonable line of enquiry.
Influenza is a contagion that strikes every winter, with symptoms of headache, fever, chill, sore throat, muscle aches, fatigue, blocked nose and cough. Severe cases lead to pneumonia, a common cause of death in the elderly. The first vaccine against influenza was produced by Ernest Williams Goodpasture at Vanderbilt University in 1931, and vaccination became widely available after the Second World War.
Flu vaccination had its first major contest with the Asian flu pandemic of 1957-1958, which killed two million worldwide. Although the vaccine failed to protect, the high mortality was attributed to insufficient coverage: the pharmaceutical industry thus turned defeat into victory. In 1960 routine flu vaccination was recommended by the US Centers for Disease Control. Each pandemic has been exploited by the pro-vaccine lobby, and as sceptic Richard Moskowitz noted, the CDC became a mouthpiece for Big Pharma.
A challenge for flu vaccine producers is the genetic volatility of the virus, which mutates rapidly. A new vaccine is needed every autumn, based on guessing which strains will emerge. These are experimental medicinal products, administered to a multitude. No more than four strains of influenza can be targeted effectively, and according to expert Jon Cohen a universal flu vaccine is no more than an ‘alchemists’ dream’.
In practice, the preventive performance of the flu jab is poor, partly due to a mismatch with the virulent strains. In 2014 the Cochrane Collaboration, an international body for evidence-based medicine, published a review comprising 25 studies with 59566 participants, revealing that flu vaccines reduced the incidence of influenza by a mere 6%. Most trials were not placebo-controlled. Tom Jefferson, one of the authors, described evidence for the efficacy of the flu vaccine as ‘rubbish’.
Nonetheless, with heavy marketing and medical hubris, uptake of the flu jab increased, particularly in the vulnerable elderly population. In 2009, health ministers across the EU agreed to a target of vaccinating 75% of older people against influenza. However, ten years later, no country had achieved this, the average being 44.3%.
Covid-19 is a coronavirus, thus not covered by flu vaccines. However, many of the risk factors for Covid-19 are the same to those stated as reasons for people to take an annual flu jab. Old age is the clearest risk factor in this pandemic, with the average age of those dying with the disease around 80. Other important factors for both flu and Covid-19 are obesity and chronic conditions such as diabetes mellitus and respiratory disease. In addition, for Covid-19 there is marked sex disparity, with men accounting for over 60% of deaths.
Compare flu vaccine frequency in older people with Covid-19 mortality by 8th May (figures from the EUand Worldometer respectively): –
Country
Flu vaccination, age 65+ (%)
Covid-19 mortality (per million)
United Kingdom
72.6
460
Netherlands
64.0
313
Portugal
60.8
109
Ireland
57.6
284*
Spain
55.7
562
Malta
55.5
11
Italy
52.0
500
France
49.7
398*
Sweden
49.4
314
Finland
47.6
47
Denmark
40.8
90
Luxembourg
37.6
160*
Germany
34.8
88*
Hungary
26.8
41
Croatia
23.0
21
Czechia
20.3
25
Romania
16.1
46
Lithuania
13.4
18
Slovakia
13.0
5
Slovenia
11.8
48
*7th May
Among countries omitted in the EU vaccination data is Belgium, which has the highest Covid-19 mortality rate in the world, at 735 per million. While specific data for older people are not readily available on the official Belgian statistics website, national population coverage indicates a relatively high flu vaccination rate in the elderly. A clear difference can be seen between east and west Europe, both in vaccine uptake and Covid-19 deaths, which may be merely coincidental.
Globally the highest uptake of the flu vaccine by seniors in 2018-2019 was in South Korea, at 83%. Third (after the UK) was the USA with 68%, and fourth was New Zealand with 67%. Neither New Zealand nor South Korea fit our hypothesis, each country having a mortality of merely 4 and 5 per million respectively. South Korea, Hong Kong, Taiwan and South Korea appear to have managed Covid-19 extremely well, despite their large populations and proximity to the source in China. Their use of tracking and tracing is impressive, and may be facilitated by cultural differences as well as technological advancement.
New Zealand’s low mortality is explained by its geographical isolation and rapid barring of entry to foreigners. Generally, the southern hemisphere has not suffered so much from Covid-19. Iceland was able to achieve similar containment. However, it appears that in continental Europe, as in North America, the virus quickly became endemic. Lockdown was like shutting the stable door after the horse had bolted.
Despite some contrary cases, it is interesting that the countries with highest death rates are Belgium, Spain, Italy, the UK, France, Netherlands, Sweden, Ireland and the USA, all having vaccinated at least half of their elderly population against flu. Denmark and Germany, with lower use of the flu vaccine, have considerably lower Covid-19 mortality. These patterns override interventions to curtail Covid-19: Sweden and Ireland have similar mortality but the former remained open for business while the other imposed strict lockdown.
Of course, correlation is not causation, and the disproportionately high Covid-19 death tolls could be explained by other factors. Western European countries and the USA have urban areas of very high population density and multicultural demography, with busy hubs of international transit. Reporting practices vary considerably between countries. However, causation of Covid-19 mortality is likely to be multifactorial, and the flu vaccine should be considered in broader post-mortem investigation of this pandemic.
Recent developments in flu vaccines may be relevant. Last autumn, the UK was the first country in Europe to introduce Flucelvax Tetra, which was touted as 36% more effective. Flu vaccines have always been produced in hens’ eggs, which are a good incubator for the virus. For the UK alone, around 50 million eggs are needed for the annual vaccine supply. The new vaccine is created in vats of cells from dogs’ kidneys. These cells are more similar to ours than those of chickens.
Vaccines have been known to give room for new resistant strains of viruses to develop, through natural selection. As reported in BMC Medicine by Alehouse and Scarpino, whooping cough outbreaks have infected vaccinated as well as unvaccinated people. As warned by critics, mandating of the chickenpox vaccine in the USA appears to have weakened the immunity gained from the naturally-acquired disease; a review by Goldman and King in Vaccine journal showed an increased incidence of shingles. Studies (e.g. Skowronski et al, 2010) indicated that people receiving the flu vaccine in one year were more likely to contract the H1N1 strain in the following year.
Vaccination against the human papilloma virus (HPV) is restricted to the two strains most linked to cervical cancer, which is likely to lead to other strains becoming prominent. In 2018 leading medical scientist Peter Gøtzsche was expelled from the Cochrane Collaboration, which he co-founded in 1993. Allegedly, he brought the organisation into disrepute after he exposed bias in a review of the HPV vaccine, which understated adverse effects.
Gøtzsche was accused of endangering millions of women by deterring vaccine uptake. In a similarly denouncing tone, British health secretary Matt Hancock stated: –
Those who campaign against vaccination are campaigning against science. The science is settled…Those who have promoted the anti-vaccination myth are morally reprehensible, deeply irresponsible and have blood on their hands.
These words do not represent a scientific attitude at all. Science is rarely ‘settled’ (a weaponising of language borrowed from climate change alarmists), certainly not in an area as complex as immunology. Just as we should be wary of anti-vaccine fundamentalists, Gøtzsche urged a critical attitude to official guidelines.
There are good reasons why people can become sceptical towards vaccines in general, or at least ask questions about them. The business practice of drug companies involves organised crime where cheating with the clinical trials and in marketing is common and has led to thousands of deaths. It is also clear that we cannot trust our drug regulators, which allow far too many dangerous drugs on to the market and are very slow to take them off again when the evidence for their lethal effects accumulates.
It has been hypothesised that vaccines may also increase susceptibility to other pathology, although this is highly contentious. Andrew Wakefield acted unethically with his research on the MMR vaccine and its putative link to inflammatory bowel disease and autism, but we should not dismiss concerns because one researcher was discredited. With the global focus on Covid-19 and the attempt to understand why some groups and nations are seemingly more susceptible to it, it is valid to ask: could the flu vaccine, while preventing certain strains of influenza, have reduced immunity to Covid-19?
Suppression of publication of research findings that contradict the accepted truth is a phenomenon well-known in climate science literature, and also in medicine, which is heavily influenced by commercial interests. And ‘the science’ is hardly robust when you consider the modelling by Neil Ferguson at Imperial College, which predicted, for example, that Sweden would have over 40 thousand deaths by the beginning of May, if it continued to refrain from a lockdown: the actual figure was fewer than three thousand.
We write not as vaccine experts but as a former chemistry teacher and a mental health lecturer. The true scientific attitude is scepticism, and that is how the orthodoxy and its assumptions are challenged. Co-author NM recently had publication of a commentary on Covid-19 refused because it didn’t concord with WHO guidelines, yet the WHO is hardly a pillar of truth, having failed to warn the world of the severity of Covid-19 in concert with the Chinese Communist Party. We should not allow institutions to thwart the search for truth or censor valid questions, however financially or politically powerful they may be.
Approximately 20% of people had an increase in antibodies against influenza in their blood after an influenza “season”. However, about three-quarters of infections were symptom-free, or so mild they weren’t identified through weekly questioning about whether participants had a cough, cold, sore throat, or a “flu-like illness”.
Traffic log cookies are used to measure site traffic. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.