- Exposure to Covid-19 is similar in Stockholm and London, based on antibody tests, despite different lockdown strategies.
- The research, published in the Journal of the Royal Society of Medicine, found that 17% of people tested in April in Stockholm had developed antibodies.
- This compares with 17% of Londoners tested in April and May, and 5%-10% of people living in Geneva.
Herd Immunity
Evidence shows we may already have developed herd immunity to COVID-19 and can continue to manage it through herd immunity.
Professor Sunetra Gupta explains herd immunity in the linked video.
Browse the articles related to this topic below.
Join our community on Guilded.
- Official data from NHS England points to a huge drop in the number of coronavirus patients being treated in hospitals today compared to mid-April, during the height of the pandemic.
- Dr Daniels: Britain is “almost reaching herd immunity”.
- Increase in hospital admissions nor a second wave to hit the UK.
- “I think that’s highly unlikely because the pubs have been open for over a month, people have been socially interacting heavily during that time, and the natural history of this disease is that if you contract the virus and you’re going to end up in hospital, you’re pretty much in hospital within 15 days of contracting it.”
Humans have never been particularly good at eradicating entire viruses, and COVID-19 might not be any different.
More than 19 million people have tested positive for the coronavirus globally, and at least 722,000 have died. In the U.S., nearly 5 million people have tested positive and more than 160,000 have died. While scientists are racing to find a cure for the virus, there’s a chance COVID-19 will never fully go away — with or without a vaccine.
Vineet Menachery, a coronavirus researcher at the University of Texas Medical Branch, told NPR’s Weekend Edition that one of the more likely scenarios is that the spread of COVID-19 will eventually be slowed as a result of herd immunity. He said that he’d be surprised “if we’re still wearing masks and 6-feet distancing in two or three years” and that in time, the virus could become no more serious than the common cold.
The first thing to remember is that we haven’t been successful at eradicating many viruses at all. Really the lone exception is smallpox, but many of these viruses exist not only in the human population but in animal populations. So coronaviruses may be removed from the human population, like SARS coronavirus in 2002, but we know that those viruses or viruses that are similar to it still exist in nature and at any time they may gain the tools to reemerge in humans again.
Fatalities are down 99% and some hospitals have no coronavirus patients, sparking hope that ‘herd immunity’ may be near
The number of people in hospital with Covid-19 has fallen 96% since the peak of the pandemic, official data reveals.
Hospital staff are now treating just 700 coronavirus patients a day in England, compared to about 17,000 a day during the middle of April, according to NHS England.
Last week, some hospitals did not have a single coronavirus patient on their wards, with one top doctor suggesting that Britain is “almost reaching herd immunity”.
https://www.thetimes.co.uk/article/covid-wards-empty-as-virus-death-toll-plunges-bvm0mxl2n
Swedish health experts say struggle against pandemic is ‘marathon not a sprint’
The country has one of the highest death rates from coronavirus in the world
Anders Tegnell’s refusal to impose lockdown is held up by critics as a warning
But is it possible the Scandinavian nation made the right call in the long-term?
- Article based on experience working as a doctor in the emergency room of one of the big hospitals in Stockholm, Sweden, and of living as a citizen in Sweden.
- Unlike other countries, Sweden never went in to complete lockdown. Non-essential businesses have remained open, people have continues to go to cafés and restaurants, children have remained in school, and very few people have bothered with face masks in public.
- COVID hit Stockholm like a storm in mid-March. One day I was seeing people with appendicitis and kidney stones, the usual things you see in the emergency room. The next day all those patients were gone and the only thing coming in to the hospital was COVID. Practically everyone who was tested had COVID, regardless of what the presenting symptom was. People came in with a nose bleed and they had COVID. They came in with stomach pain and they had COVID.
- Then, after a few months, all the COVID patients disappeared.
- At the peak three months back, a hundred people were dying a day of COVID in Sweden, a country with a population of ten million. We are now down to around five people dying per day in the whole country, and that number continues to drop. Since people generally die around three weeks after infection, that means virtually no-one is getting infected any more.
- The risk of dying is at the very most 1 in 200 if you actually do get infected.
- In total COVID has killed under 6,000 people in a country of ten million.
- Sweden has an annual death rate of around 100,000 people. Considering that 70% of those who have died of COVID are over 80 years old, quite a few of those 6,000 would have died this year anyway.
- COVID will never even come close to major pandemic numbers like 1918 flu.
- If herd immunity hasn’t developed, where are all the sick people? Why has the rate of infection dropped so precipitously?
- The reason we test for antibodies is because it is easy and cheap. Antibodies are in fact not the body’s main defence against virus infections. T-cells are. But T-cells are harder to measure than antibodies, so we don’t really do it clinically.
- Sweden ripped the metaphorical band-aid off quickly and got the epidemic over and done with in a short amount of time, while the rest of the world has chosen to try to peel the band-aid off slowly.
- I am willing to bet that the countries that have shut down completely will see rates spike when they open up. If that is the case, then there won’t have been any point in shutting down in the first place, because all those countries are going to end up with the same number of dead at the end of the day anyway. Shutting down completely in order to decrease the total number of deaths only makes sense if you are willing to stay shut down until a vaccine is available. That could take years.
- COVID has at present killed less than 6000 in Sweden. It is very unlikely that the number of dead will go above 7,000. An average influenza year in Sweden, 700 people die of influenza. Does that mean COVID is ten times worse than influenza? No, because influenza has been around for centuries while COVID is completely new.
- So it is quite possible, in fact likely, that the case fatality rate for COVID is the same as for influenza, or only slightly higher, and the entire difference we have seen is due to the complete lack of any immunity in the population at the start of this pandemic.
Original source: https://sebastianrushworth.com/2020/08/04/how-bad-is-covid-really-a-swedish-doctors-perspective/
But with no sign of a second summer wave nor an autumn eruption reminiscent of 1918, the commentariat has amended the definition. Suddenly, a “second wave” meant Covid’s seasonal return, in winter, a year on. Widespread adoption of a new phrase in the Covid lexicology – “winter wave” – has academically formalised the idea.
But instead of looking us square in the eye, the Tories have chosen Big Brother’s panopticon; No 10’s new Joint Biosecurity Centre, which will drive “whack-a-mole” local lockdowns, is slickness posing as strategy – and, as it happens, reporting into track-and-trace app failure Dido Harding. When the public twigs that the infection is unlikely to be controlled in this way, the sheer panic could send us back into national lockdown. Three scenarios might help avoid the latter: a vaccine comes along; the Government gets its act together with a plan to protect the vulnerable; or we put in place safety valves against mass hysteria.
Imperial College’s research needs to be particularly scrutinised, as its international influence grows. Dr Seth Flaxman – the first author in the paper that notoriously claimed lockdowns may have prevented over 3 million deaths in Europe – this week won fresh funding to model the pandemic across several countries.
Revelations that disrupt the narrative also need to find a stronger voice: within 24 hours, the scandal of PHE’s inflated daily death figures was running out of mileage. This week’s London School of Hygiene and Tropical Medicine modelling on the impact of the pandemic on cancer deaths never gathered steam. So too a paper by Oxford’s Prof Sunetra Gupta, which elegantly combined those uneasy epidemiological bedfellows – theory and evidence – to find some parts of the UK may already have reached herd immunity.
“Intensive care units are getting empty, the wards are getting empty, we are really seeing a decrease — and that despite that people are really loosening up. The beaches are crowded, social distancing is not kept very well … but still the numbers are really decreasing. That means that something else is happening – we are actually getting closer to herd immunity. I can’t really see another reason.”
“I can’t say if the Swedish approach was right or wrong – I think we can say that in one or two years when we are looking back. You have to look at the mortality over the whole period.”
“I don’t think that we have more new cases, I think we are just detecting more cases”
“We found that if you have a mild case you can be negative for antibodies afterwards … in those almost all of them had strong T-cell activity. This study says that there are cases that you can have a strong T-cell response even though you have not had antibodies, meaning that you have encountered the virus and built up immunity.”
“[R]oughly twice as many people have developed T-cell immunity compared with those who we can detect antibodies in.“
SARS-CoV-2-specific memory T cells will likely prove critical for long-term immune protection against COVID-19. We systematically mapped the functional and phenotypic landscape of SARS-CoV-2-specific T cell responses in a large cohort of unexposed individuals as well as exposed family members and individuals with acute or convalescent COVID-19. Acute phase SARS-CoV-2-specific T cells displayed a highly activated cytotoxic phenotype that correlated with various clinical markers of disease severity, whereas convalescent phase SARS-CoV-2-specific T cells were polyfunctional and displayed a stem-like memory phenotype. Importantly, SARS-CoV-2-specific T cells were detectable in antibody-seronegative family members and individuals with a history of asymptomatic or mild COVID-19. Our collective dataset shows that SARS-CoV-2 elicits robust memory T cell responses akin to those observed in the context of successful vaccines, suggesting that natural exposure or infection may prevent recurrent episodes of severe COVID-19 also in seronegative individuals.
https://www.biorxiv.org/content/10.1101/2020.06.29.174888v1.full
Interview highlights:
- We have already developed herd immunity to COVID-19 and will continue to manage it through herd immunity.
- Flu is much more dangerous than COVID-19.
- COVID-19 will settle into an endemic state just like flu.
- Hopefully vaccines will be important in protecting the vulnerable.
- Another way to protect the vulnerable sector is to allow the population to develop natural immunity.
- There’s no reason to think the virus will mutate into a lower level of virulence.
- During the 1918 flu because of a large number of ‘immunologically naive’ individuals but this is not the case with COVID-19.
- Most of us have some degree of coronavirus immunity and therefore some protection to COVID-19.
- The current H1 influenza strain is antigenically identical to the 1918 flu. H1 flu doesn’t kill as many people as the 1918 flu because most people already have cross immunity.
Mirror:
Antibody tests on random samples of the population have so far shown much lower levels of general infection than the government’s scientific advisers claimed would be necessary to attain ‘herd immunity’. In London, for example, tests have shown that 17 per cent of the population have antibodies to Sars-CoV-2, the virus that causes Covid-19. In New York, the figure is 21 per cent. At the beginning of this crisis, on the other hand, Sir Patrick Vallance, the chief scientific adviser, suggested that at least 60 per cent of the population would have to be infected in order to achieve herd immunity.
https://www.spectator.co.uk/article/is-covid-immunity-more-common-than-we-think-
Naturally acquired herd immunity to COVID-19 combined with earnest protection of the vulnerable elderly – especially nursing home and assisted living facility residents — is an eminently reasonable and practical alternative to the dubious panacea of mass compulsory vaccination against the virus.
This strategy was successfully implemented in Malmo, Sweden, which had few COVID-19 deaths by assiduously protecting its elder care homes, while “schools remained open, residents carried on drinking in bars and cafes, and the doors of hairdressers and gyms were open throughout.
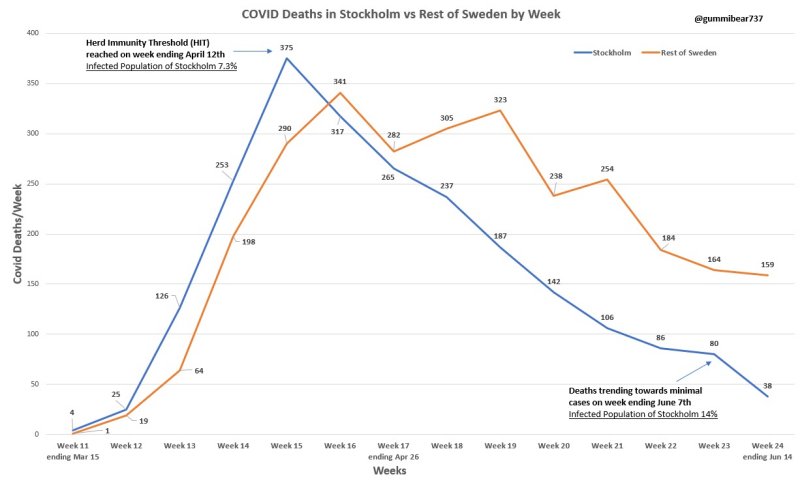
@gummibear737, a Twitter use who has been analysing COVID-19 data, has published a chart that confirms a hypothesis by Dr Michael Levitt:
Stockholm is the best population to test Covid theory whereby it was hit hard early and did not have lockdowns. Nobel Prize winner Dr Michael Levitt postulated that the virus burns out when it has infected 15-20% of the population. According to this, he’s right.
So what does this mean? Lockdowns were a waste of time and resources. Minimizing deaths just delays the inevitable. Those countries which were not hit are most likely to see continued spikes and outbreaks. Maybe less during the summer but a second wave later this year.
Up to 81% of of the population can mount a strong response to COVID-19 without ever having been exposed to it before:
Cross-reactive SARS-CoV-2 T-cell epitopes revealed preexisting T-cell responses in 81% of unexposed individuals, and validation of similarity to common cold human coronaviruses provided a functional basis for postulated heterologous immunity
The SARS-CoV-2 pandemic calls for the rapid development of diagnostic, preventive, and therapeutic approaches. CD4+ and CD8+ T cell-mediated immunity is central for control of and protection from viral infections[1-3]. A prerequisite to characterize T-cell immunity, but also for the development of vaccines and immunotherapies, is the identification of the exact viral T-cell epitopes presented on human leukocyte antigens (HLA)[2-8]. This is the first work identifying and characterizing SARS-CoV-2-specific and cross-reactive HLA class I and HLA-DR T-cell epitopes in SARS-CoV-2 convalescents (n = 180) as well as unexposed individuals (n = 185) and confirming their relevance for immunity and COVID-19 disease course. SARS-CoV-2-specific T-cell epitopes enabled detection of post-infectious T-cell immunity, even in seronegative convalescents. Cross-reactive SARS-CoV-2 T-cell epitopes revealed preexisting T-cell responses in 81% of unexposed individuals, and validation of similarity to common cold human coronaviruses provided a functional basis for postulated heterologous immunity[9] in SARS-CoV-2 infection[10,11]. Intensity of T-cell responses and recognition rate of T-cell epitopes was significantly higher in the convalescent donors compared to unexposed individuals, suggesting that not only expansion, but also diversity spread of SARS-CoV-2 T-cell responses occur upon active infection. Whereas anti-SARS-CoV-2 antibody levels were associated with severity of symptoms in our SARS-CoV-2 donors, intensity of T-cell responses did not negatively affect COVID-19 severity. Rather, diversity of SARS-CoV-2 T-cell responses was increased in case of mild symptoms of COVID-19, providing evidence that development of immunity requires recognition of multiple SARS-CoV-2 epitopes. Together, the specific and cross-reactive SARS-CoV-2 T-cell epitopes identified in this work enable the identification of heterologous and post-infectious T-cell immunity and facilitate the development of diagnostic, preventive, and therapeutic measures for COVID-19.
All through the Covid-19 pandemic we have been hampered by a lack of data on just how many people have had the disease. Given that several studies have indicated that as many as 80 per cent of people who are infected show no symptoms whatsoever, it is extremely difficult to estimate this crucial figure – which determines the mortality rate of Covid-19 and also how far away we might be from achieving a position of herd immunity.
Today, however, comes some very substantial data. The Medical Research Council’s Biostatistics Unit has published estimates of infections derived from serological studies on samples collected from the NHS Blood Transfusion Service.
https://www.spectator.co.uk/article/one-in-ten-brits-may-have-had-coronavirus
One of the key things about science – obvious to its practitioners, but often obscure to outsiders – is that it is fuelled by doubt, not certainty. When the ‘facts’ change (as they often do), and when original assumptions are qualified or overturned, then any scientist worth their salt re-examines and, if necessary, alters their conclusions. The presence of cross-reactive helper cells in maybe half the population means that ideas about a possible second wave must be rewritten. This finding must make a second wave less likely, probably much less likely. And the fact that there has been no ‘second wave’ (as opposed to isolated outbreaks) anywhere where lockdown has been released also fits this hypothesis. It may well also explain why the first wave didn’t infect much higher proportions of the population.
https://www.spectator.co.uk/article/science-doubt-and-the-second-wave-of-covid
Note: The video has been removed from Vimeo but has been archived on BitChute (see embedded below highlights).
James talks with Professor Dolores Cahill, a world renowned immunologist who has advised the Irish government and the EU.
- We should end the lockdown. Quarantining healthy people was a huge mistake, should never have been done and should never happen again.
- All the available information tells us there’s no longer any basis for the lockdowns. The economic harm and resulting health effects could be five times higher than those caused by the virus. The adverse health implications of poverty is well-known and has lots of supporting data.
- The immunology community knew in January and February that there was nothing very special about COVID-19.
- There are lots of clinical trials showing the usefulness of vitamins C, D and Zinc for preventing symptoms of corona-type viruses.
- It is also very well established that hydroxychloroquine, which is a very safe drug, can be used as a treatment.
- There was no need to ramp up the hospital care system because there were established methods for prevention and treatment.
- It was known that the virus would circulate the world in a month. Professor Cahill was surprised at the lockdown because the ‘virus was gone.’ There is clearly enough data for this.
- COVID-19 (also known as SARS-CoV-2) is about 80% the same as SARS-CoV-1 in 2003. These types of viruses last about 6 weeks in each location before naturally ‘dying off’ as people become exposed and then developing immunity.
- 80 out of 100 people would have developed antibodies within 10-11 days and become immune for life without experiencing symptoms.
- Although COVID-19 is a novel virus, it can be ‘recognized’ by the immune system of anyone who had already been exposed to SARS-CoV-1. This is because of COVID-19’s 80% similarity to the earlier 2003 virus.
- With these types of viruses, you will be negative for the PCR test (which tests for the presence of the virus) after recovery but you will test positive for the antibodies.
- You don’t need the lockdown if you boost your immune system. in fact, the lockdown made matters worse by depressing people’s immune system. Sunshine, interacting with people, shaking hands–all these help to boost your immune system.
- Elderly people should be taking vitamin C, D and Zinc to protect their immune systems. People with underlying conditions, or those who develop symptoms, should contact their doctor to consider prescribing off-label hydroxychloroquine.
- Symptoms: flu-like for the first five days. If it gets worse and you develop a cough, that’s when you need to ring your doctor for treatment. Treatment includes hydroxychloroquine for 3-5 days, with Zinc and AZT antibiotic. This is an established protocol that has been used in many clinical trials in 2020.
- There was some reason to be scared of COVID-19 during the very early stages (around January) because because we didn’t know anything about it. However, the media and WHO was fearmongering when they used Wuhan as an example of what would happen everywhere.
- From February onward, the immunology community recognized that COVID-19 is the same as a normal virus in most parts of the world. There was something different about Wuhan, Bergamo and New York but t here was no reason to lockdown the rest of the world.
- Vaccines have their place and can be safe. However, studies show that animal and human subjects that were given a type of influenza vaccine later reacted badly when they encountered a coronavirus ‘in the wild’. The reaction caused a cytokine storm that either killed the subject or made the subject very ill. The reaction between different types of vaccinated and wild viruses is called viral interference.
- People in Wuhan and Bergamo were given a certain type of influenza vaccine. It became apparent around April-May that the high death rates in both cities could be due to viral interference from the administered influenza vaccine.
- It has not been possible to make a safe and effective vaccine for the SARS-CoV-1 in 2003. If we have not been able to make a vaccine for this coronavirus, we should not expect a safe vaccine for COVID-19 any time soon. A vaccine developed for COVID-19 would be a complete experiment on those who take it.
- Vaccines containing alluminium, Thimerodal or mercury are intrinsically unsafe.
- The global death rate for COVID-19 is around the same as a bad influenza. Outside of Wuhan, Bergamo and New York, the death rate appears to be less than the normal flu.
- Current data shows that the real death rate for COVID-19 is 20 or 30 times less than the initial estimates from the WHO. We now know the death rate is about one in a thousand for the vulnerable and one in five thousand for the healthy. In the under 70s age range, this is lower than the average flu.
- It was well-known in February that there was no need for the lockdowns.
- There have been no cases of transmission from children.
- If we were to end the lockdown, we would need 10 days to prepare. This is because people have not been out and exposed to sunlight. Preparation include taking vitamins C, D and Zinc; getting fresh air; avoiding stress; and making sure doctors have hydroxychloroquine.
- It is almost as if the current advice is geared to making sure people get sick in order to support more lockdowns.
- There will be no second spike if people take the above precautions to strengthen their immune system.
- A recent study shows that people who continued working were healthy. Engaging with other keeps you healthy by strengthening the immune system.
- There hasn’t been an open debate in any country about the harm versus benefits of the lockdown. This may be a big reason for why the lockdowns are continuing.
- Dr. Rashid A. Buttar and Dr. Judy Mikovits are trying to open the debate about prevention and treatments but their voices are being censored.
- The use of hydroxychloroquine as a treatment has been politicized.
- Evidence is being cherry-picked in order reach a predetermined goal: a money-making vaccine. The existing prevention and treatment methods don’t make money for big-pharma.
- Masks and social distancing is appropriate for something like ebola but not for coronaviruses.
- We will build up herd immunity within about two weeks.
- We know how COVID-19 is transmitted because it belongs to the family of coronaviruses. It is not transmitted through the air. This has been proven because groups of people in encloses spaces (for example, plane-loads of fruit-pickers) did not all come down with the sickness.
- The two meter rule is unnecessary.
- There was enough information from many sources for the government and their advisors to know that all these measures are wrong. There should be legal implications for those who advocate continued lockdown. Hundreds of unnecessary deaths should be grounds for a legal tribunal.
- There is a high risk of a death spike after lockdown due to other causes, such as cancers, that will attributed to COVID-19. This will be used to support more lockdowns.
- The politicians, broadcasters, newspaper editors, ministers for health–everyone complicit in censoring and withholding information from the public about the true nature of COVID-19 needs to be held personally liable for the deaths caused.
“It’s becoming clear that a lot of people have been exposed to the virus and that the death rate in people under 65 is not something you would lock down the economy for,” she says. “We can’t just think about those who are vulnerable to the disease. We have to think about those who are vulnerable to lockdown too. The costs of lockdown are too high at this point.”
Asymptomatic SARS-CoV-2 infection is common and can be detected by analysis of saliva or NTS. NTS viral loads fall faster in asymptomatic individuals, but they appear able to transmit the virus to others.
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa711/5851471
Professor Karl Friston is a computer modelling expert, world-renowned for his contributions to neuroscience. He has been applying his “dynamic causal modelling” approach to the Covid-19 pandemic, and has reached some startling results.
– The differences between countries are not primarily down to government actions, but due to ‘intrinsic’ differences in the populations
– We don’t yet fully understand what is driving it, although there are theories ranging from levels of vitamin D to genetic differences
– In each country, there appears to be a portion of the population that is ‘not even in the game’ – that is, not susceptible to Covid-19. This varies hugely between countries
– In the UK, Professor Friston estimates that portion to be at least 50%, and probably more like 80%
– The similar mortality results between Sweden (no lockdown) and the UK (lockdown) are best explained by the fact that in reality there was no difference
– the impact of the legal lockdown in Professor Friston’s models “literally goes away”.