Around one-third of hospital deaths during the initial COVID-19 peak were due to inappropriate treatment.
“We were intubating sick patients very early. Not for the patients’ benefit, but in order to control the epidemic & to save other patients,” Dr. Iwashyna said “That felt awful.”
…As a safety precaution, doctors and hospitals limited the access of health-care workers to coronavirus patients on ventilators, giving them fewer opportunities to check on them. That meant patients required more powerful sedatives to keep them from pulling out throat tubes.
…Overall, survival for Covid-19 patients increased 28% from April to September at HCA hospitals.
…Before the pandemic, between about 30% to more than 40% of ventilator patients died, according to research. Numbers were sharply higher in Wuhan, China. As the pandemic grew, hospitals in the U.S. reported death rates in some cases of about 50% for ventilated Covid-19 patients.
December 9 – UK authorities confirmed 2 cases of anaphylaxis after vaccination
December 18*, 2020 – CDC has identified 6 case reports of anaphylaxis following Pfizer-BioNTech vaccine meeting Brighton Collaboration criteria for anaphylaxis
Persons with anaphylaxis following COVID-19 vaccination should not receive additional doses of COVID-19 vaccine
A hospital worker with no history of allergies was admitted to intensive care over a severe reaction she suffered 10 minutes after having Pfizer’s coronavirus vaccine. The unidentified female worker suffered an anaphylactic reaction shortly after receiving the injection at a hospital in Juneau, Alaska, on Tuesday.
Two healthcare workers in the UK suffered an anaphylactic reaction to the Pfizer injection after being given it last week, although the vaccine has been widely tested and analysed, with government experts in both the US and Great Britain deeming it safe.
More than 100,000 patients will not be able to get the Covid vaccine from their family doctor after their GP surgeries decided not to take part in its deployment, the Guardian can reveal.
“We fully support the swine flu vaccination programme … The vaccine has been thoroughly tested,” they declared in a joint statement.
Except, it hadn’t. Anticipating a severe influenza pandemic, governments around the world had made various logistical and legal arrangements to shorten the time between recognition of a pandemic virus and the production of a vaccine and administration of that vaccine in the population. In Europe, one element of those plans was an agreement to grant licences to pandemic vaccines based on data from pre-pandemic “mock-up” vaccines produced using a different virus (H5N1 influenza). Another element, adopted by countries such as Canada, the US, UK, France, and Germany, was to provide vaccine manufacturers indemnity from liability for wrongdoing, thereby reducing the risk of a lawsuit stemming from vaccine related injury.
COVID-19 vaccines designed to elicit neutralising antibodies may sensitise vaccine recipients to more severe disease than if they were not vaccinated. Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralising antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID-19 disease via antibody-dependent enhancement (ADE). This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID-19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
Most people will escape “severe” side effects, defined as those that prevent daily activity. Fewer than 2% of recipients of the Pfizer and Moderna vaccines developed severe fevers of 39°C to 40°C. But if the companies win regulatory approvals, they’re aiming to supply vaccine to 35 million people worldwide by the end of December. If 2% experienced severe fever, that would be 700,000 people.
Other transient side effects would likely affect even more people. The independent board that conducted the interim analysis of Moderna’s huge trial found that severe side effects included fatigue in 9.7% of participants, muscle pain in 8.9%, joint pain in 5.2%, and headache in 4.5%. In the Pfizer/BioNTech vaccine trial, the numbers were lower: Severe side effects included fatigue (3.8%) and headache (2%).
But that’s a higher rate of severe reactions than people may be accustomed to. “This is higher reactogenicity than is ordinarily seen with most flu vaccines, even the high-dose ones,” says Arnold Monto, an epidemiologist at the University of Michigan School of Public Health.
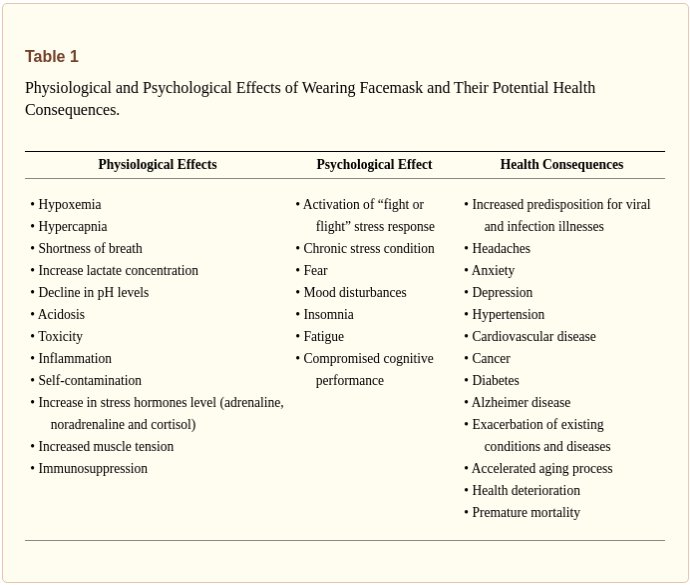
Many countries across the globe utilized medical and non-medical facemasks as non-pharmaceutical intervention for reducing the transmission and infectivity of coronavirus disease-2019 (COVID-19). Although, scientific evidence supporting facemasks’ efficacy is lacking, adverse physiological, psychological and health effects are established. Is has been hypothesized that facemasks have compromised safety and efficacy profile and should be avoided from use. The current article comprehensively summarizes scientific evidences with respect to wearing facemasks in the COVID-19 era, providing prosper information for public health and decisions making.
…Thedata suggest that both medical and non-medical facemasks are ineffective to block human-to-human transmission of viral and infectious disease such SARS-CoV-2 and COVID-19, supporting against the usage of facemasks. Wearing facemasks has been demonstrated to havesubstantial adverse physiological and psychological effects.
Two major U.S. pharmaceutical companies racing to develop novel coronavirus vaccines have announced that their vaccines have been confirmed to be over 90% effective. But Masayuki Miyasaka, a leading immunologist at Osaka University, told the Mainichi Shimbun in a recent interview that even after these vaccines become available, he does not plan to receive them for the time being.
At a meeting of the Committee on Health, Labor and Welfare of Japan’s House of Representatives on Nov. 17, Miyasaka stated, “There’s no doubt that their effectiveness is quite high, but their safety is not guaranteed at all,” sounding a word of caution about expectations for the vaccines.
TED (Tenders Electronic Daily) is the online version of the ‘Supplement to the Official Journal’ of the EU, dedicated to European public procurement.
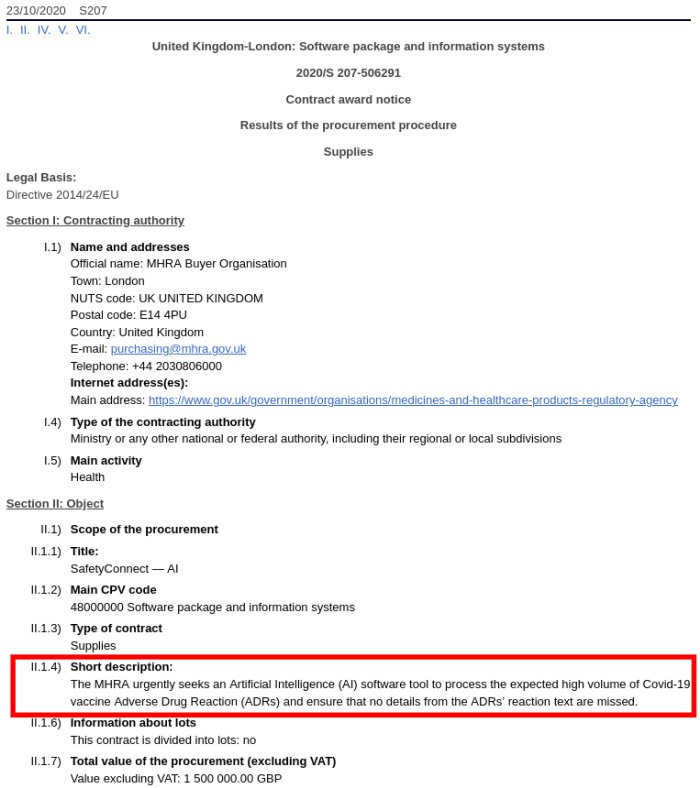
The MHRA urgently seeks an Artificial Intelligence (AI) software tool to process the expected high volume of Covid-19 vaccine Adverse Drug Reaction (ADRs) and ensure that no details from the ADRs’ reaction text are missed.
Masks have been shown consistently over time and throughout the world to have no significant preventative impact against any known pathogenic microbes. Specifically, regarding COVID-19, we have shown in this paper that mask use is not correlated with lower death rates nor with lower positive PCR tests.
Masks have also been demonstrated historically to contribute to increased infections within the respiratory tract. We have examined the common occurrence of oral and nasal pathogens accessing deeper tissues and blood, and potential consequences of such events. We have demonstrated from the clinical and historical data cited herein, we conclude the use of face masks will contribute to far more morbidity and mortality than has occurred due to COVID-19.
We call for collaborative efforts from scientists, manufacturers, and regulators to assess such risks and look for viable methods to reducing micro(nano)plastics and other respirable debris in face masks and respirators worn by a large population worldwide during the current pandemic.
A curated list of mask facts and medical publications.
COVID-19 is as politically-charged as it is infectious. Early in the COVID-19 pandemic, the WHO, the CDC and NIH’s Dr. Anthony Fauci discouraged wearing masks as not useful for non-health care workers. Now they recommend wearing cloth face coverings in public settings where other social distancing measures are hard to do (e.g., grocery stores and pharmacies). The recommendation was published without a single scientific paper or other information provided to support that cloth masks actually provide any respiratory protection. Let’s look at the data.
Surgical masks are loose fitting. They are designed to protect the patient from the doctors’ respiratory droplets. There wearer is not protected from others’ airborne particles.
People do not wear masks properly. Many people have the mask under the nose. The wearer does not have glasses on and the eyes are a portal of entry. If the virus lands on the conjunctiva, tears will wash it into the nasopharynx.
Most studies cannot separate out hand hygiene.
The designer masks and scarves offer minimal protection. They give a false sense of security to both the wearer and those around the wearer. **Not to mention they add a perverse lightheartedness to the situation.
If you are walking alone, no need for a mask. Avoid other folks; use common sense.
Remember: children under 2 years should not wear masks because of accidental suffocation and difficulty breathing in some.
Even if a universal mask mandate were imposed, several studies noted that folks do not use the mask properly and over-report their wearing. Additionally, how would the mandate be enforced??
The positive studies are models that assume universality and full compliance.
If wearing a mask makes people go out and get Vitamin D – go for it. In the 1918 flu pandemic people who went outside did better. Early reports are showing people with COVID-19 with low Vitamin D do worse than those with normal levels. Perhaps that is why shut-ins do so poorly.
Masks and gloves have been shown in studies to help in the medical setting but not in the home setting.
Cloth masks are worse and may increase infection.
Masks in the UK were supposed to reduce infections by 40% but in fact, infections went up.
Study in Norway: 200,000 people would have to wear a mask in order to prevent one infection. Public health impact of mask wearing is negligible.
This advocating mask-wearing have cherry-picked low-quality observational evidence to suit the evidence.
Carl Heneghan is a clinical epidemiologist with expertise in evidence-based medicine, research methods, and evidence synthesis. He is Director of the NIHR SPCR Evidence Synthesis Working Group a collaboration of nine primary care departments across UK universities. He set up and directs the Oxford COVID Evidence Service, has over 400 peer-reviewed publications (current H Index 67); published 95 systematic reviews. He is Editor in Chief of BMJ Evidence-Based Medicine, and Editor of the Catalogue of Bias.
Director of CEBM & Programs in EBHC Editor in Chief, BMJ EBM NHS Urgent Care GP NIHR Senior Investigator
California Globe has seen reports of lung infections from long-term mask wearing, persistent coughing, as well as dermatitis on the skin around the mouth.
Providing one more reason healthy people should not wear face masks, Dentists report they are seeing a new syndrome brought about by mask-wearing which the doctors have dubbed “mask mouth,” Fox News reports.
The moisture trapped in face masks creates a petri dish of breeding ground for bacteria, as it is in place directly over your mouth.
Constant mask-wearing “is leading to all kinds of dental disasters like decaying teeth, receding gum lines and seriously sour breath.
“We’re seeing inflammation in people’s gums that have been healthy forever, and cavities in people who have never had them before,” says Dr. Rob Ramondi, a dentist and co-founder of One Manhattan Dental. “About 50% of our patients are being impacted by this, [so] we decided to name it ‘mask mouth’ — after ‘meth mouth.’ ”
Abstract Objectives: This study was undertaken to evaluate whether the surgeons’ oxygen saturation of hemoglobin was affected by the surgical mask or not during major operations.
Methods: Repeated measures, longitudinal and prospective observational study was performed on 53 surgeons using a pulse oximeter pre and postoperatively.
Results: Our study revealed a decrease in the oxygen saturation of arterial pulsations (SpO2) and a slight increase in pulse rates compared to preoperative values in all surgeon groups. The decrease was more prominent in the surgeons aged over 35.
Conclusions: Considering our findings, pulse rates of the surgeon’s increase and SpO2 decrease after the first hour. This early change in SpO2 may be either due to the facial mask or the operational stress. Since a very small decrease in saturation at this level, reflects a large decrease in PaO2, our findings may have a clinical value for the health workers and the surgeons.
In July Health Secretary Matt Hancock claimed that conspiracy theorists are putting lives at risk
The UK government’s Vaccine Damage Payment scheme is proof that vaccines can be unsafe
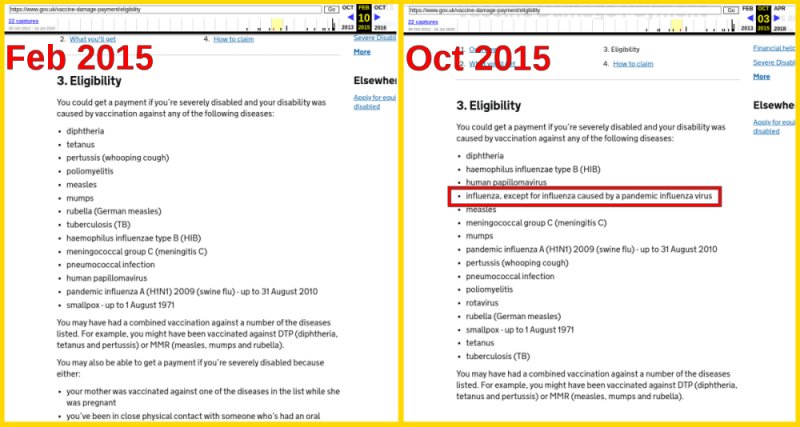
Eligibility criteria Vaccine Damage Payment changed in 2015
Update October 2020: AstraZeneca protected from vaccine liability
Update November 2020: MHRA expects high volume of COVID-19 vaccine adverse drug reaction
Update December 2020: Pfizer is given protection from legal action by the UK government
Discussion around vaccinations can be very contentious. There’s great nuance in this area and a short post will not do justice to the complex issues surrounding the usefulness and safety of vaccines. Nevertheless, while vaccines may have their role in protecting target populations from disease, not all have been proven safe to an acceptable level as shown in the resources below.
The UK government’s Vaccine Damage Payment scheme is probably the strongest proof that vaccines can be unsafe. Under the Vaccine Damage Payment scheme, people who have been severely disabled as a result of a vaccination against certain diseases can be eligible for a one-off tax-free payment of £120,000.
Conspiracy theorists are putting lives at risk?
It is an objective fact that a compensation scheme exists for those who have been damaged by vaccines. Nevertheless, Health Secretary Matt Hancock claimed that conspiracy theorists are putting lives at risk:
“Those who promulgate lies about dangers of vaccines that are safe and have been approved–they are threatening lives…”
Clearly, concerns about the safely of vaccines cannot be lies if there is a vaccine damage compensation scheme in place.
Eligibility changed in 2015
Eligibility requirements for vaccines covering certain diseases are listed and change over time. Interestingly, sometime around 2015, damage from vaccines for influenza caused by pandemics are explicitly listed as not eligible.
We do not know how the government compiles is eligibility criteria or why this change was made. However, it would be worthwhile to keep an eye on this list to see if the status of the upcoming COVID-19 vaccines.
AstraZeneca protected from vaccine liability
Update 1 August 2020: On 30 July 2020, Reuters reported that AstraZeneca, the UK government’s partner for developing its COVID-19 vaccine, will be exempt from coronavirus vaccine liability claims in most countries. The countries have not been named but Ruud Dobber, a member of Astra’s senior executive team, commented:
“This is a unique situation where we as a company simply cannot take the risk if in … four years the vaccine is showing side effects.
In the contracts we have in place, we are asking for indemnification. For most countries it is acceptable to take that risk on their shoulders because it is in their national interest.”
MHRA expects high volume of COVID-19 vaccine adverse drug reaction
Update November 2020: It came to light in mid-November that the UK’s Medicines & Healthcare products Regulatory Agency (MHRA) put out a contract award notice for an Artificial Intelligence (AI) software tool. It appears they expect a high volume of COVID-19 vaccine Adverse Drug Reaction (ADRs) from the upcoming vaccines:
…it is not possible to retrofit the MHRA’s legacy systems to handle the volume of ADRs that will be generated by a Covid-19 vaccine. Therefore, if the MHRA does not implement the AI tool, it will be unable to process these ADRs effectively.
Pfizer given legal indemnity
Update 2 December 2020:According to the Independent, Pfizer now has a legal indemnity from being sued by patients who develop any complications from its new mRNA vaccine that will be rolled out in the UK. NHS staff providing the vaccine will also be protected.
AstraZeneca has been granted protection from future product liability claims related to its COVID-19 vaccine hopeful by most of the countries with which it has struck supply agreements, a senior executive told Reuters.
Background Medical masks are commonly used in health care settings to protect healthcare workers (HCWs) from respiratory and other infections. Airborne respiratory pathogens may settle on the surface of used masks layers, resulting in contamination. The main aim of this study was to study the presence of viruses on the surface of medical masks.
Methods Two pilot studies in laboratory and clinical settings were carried out to determine the areas of masks likely to contain maximum viral particles. A laboratory study using a mannequin and fluorescent spray showed maximum particles concentrated on upper right, middle and left sections of the medical masks. These findings were confirmed through a small clinical study. The main study was then conducted in high-risk wards of three selected hospitals in Beijing China. Participants (n = 148) were asked to wear medical masks for a shift (6–8 h) or as long as they could tolerate. Used samples of medical masks were tested for presence of respiratory viruses in upper sections of the medical masks, in line with the pilot studies.
Results Overall virus positivity rate was 10.1% (15/148). Commonly isolated viruses from masks samples were adenovirus (n = 7), bocavirus (n = 2), respiratory syncytial virus (n = 2) and influenza virus (n = 2). Virus positivity was significantly higher in masks samples worn for > 6 h (14.1%, 14/99 versus 1.2%, 1/49, OR 7.9, 95% CI 1.01–61.99) and in samples used by participants who examined > 25 patients per day (16.9%, 12/71 versus 3.9%, 3/77, OR 5.02, 95% CI 1.35–18.60). Most of the participants (83.8%, 124/148) reported at least one problem associated with mask use. Commonly reported problems were pressure on face (16.9%, 25/148), breathing difficulty (12.2%, 18/148), discomfort (9.5% 14/148), trouble communicating with the patient (7.4%, 11/148) and headache (6.1%, 9/148).
Conclusion Respiratory pathogens on the outer surface of the used medical masks may result in self-contamination. The risk is higher with longer duration of mask use (> 6 h) and with higher rates of clinical contact. Protocols on duration of mask use should specify a maximum time of continuous use, and should consider guidance in high contact settings. Viruses were isolated from the upper sections of around 10% samples, but other sections of masks may also be contaminated. HCWs should be aware of these risks in order to protect themselves and people around them.
Traffic log cookies are used to measure site traffic. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.