- 2.4% of all tests were positive (9,674 out of 397,197)
- 3.9% of residents tested positive (6,747 out of 172,066)
- 3.3% of asymptomatic residents tested positive (5,455 out of 163,945)
- 80.9% of residents who tested positive were asymptomatic (5,455 out of 6,747)
- 1.2% of asymptomatic staff tested positive (2,567 out of 210,620)
Elderly
Browse the articles related to this topic below.
Join our community on Guilded.
Lockdown deaths:
The really concerning thing is that if all the deaths taking place during lockdown are put down as Covid-19 deaths, we are going to miss the fact that the lockdown policies have caused an increase in deaths from many other things. There has been a 50 per cent reduction in people turning up to A&E. It is clear that people just do not want to bother the doctors. And a number of these people will be dying. If we muddle the Covid-19 statistics in with the other statistics, we might think the lockdown has prevented a certain number of deaths, when it has actually caused a large number of deaths.
NHS capacity:
You hear this idea that all NHS staff have been working 20 times as hard as they have ever done. This is complete nonsense. An awful lot of people have been standing around wondering what the hell to do with themselves. A&E has never been so quiet.
The chances of children dying from COVID-19:
How many people aged 15 or under have died of Covid-19? Four. The chance of dying from a lightning strike is one in 700,000. The chance of dying of Covid-19 in that age group is one in 3.5million. And we locked them all down. Even among the 15- to 44-year-olds, the death rate is very low and the vast majority of deaths have been people who had significant underlying health conditions. We locked them down as well. We locked down the population that had virtually zero risk of getting any serious problems from the disease, and then spread it wildly among the highly vulnerable age group.
On vaccines:
It is not clear that getting the virus actually makes you immune to it in the future, and it is not clear a vaccine would either.
https://www.spiked-online.com/2020/06/26/the-lockdown-is-causing-so-many-deaths/
Laura Dodsworth interviews Alistair Haimes on Freethinking with Laura Dodsworth.
Support Laura Dodsworth through Patreon:
https://www.patreon.com/lauradodsworth
Interview notes and charts
- The difference between what the government was telling us and what their information was telling us was so extreme and outrageous.
- Exponential means a “constant rate of growth.” The government data in March was clearly showing that the COVID-19 was declining, not growing exponentially. This was the same in all countries you could see the data. [See chart 1]
- A constantly declining growth rate will make a bell curve. The government were standing in front of bell curve graphs during their briefings yet they were telling us we were in the middle of the epidemic.
- It was very clear that we were heading to a peak sometime around early to mid-April.
- You don’t have to be complicated mathematics to see that COVID-19 was running out of steam almost from day one.
- The conclusion from the Centre for Evidence-Based Medicine seems to be that it’s impossible to predict if there will be a second wave.
- Sweden’s epidemic looks identical to the UK’s but they did not lockdown. Their datapoint indicates there won’t be a second wave. There has been no spike in Denmark either. [See chart 2]
- Unknowns: has summer affected COVID-19 and will there be a mutation?
- Will illnesses during the autumn and winter be mis-attributed to COVID-19? Poor media coverage means that we can’t be sure.
- Symptoms of COVID-19 are very similar to the flu. Something could look like a second wave but will we really know?
- The lockdown is costing a Brexit bill a week.
- The government response seems to have been skewed by Neil Ferguson’s modelling data. The make-up of government advisors seems to be a recipe for groupthink, which is very dangerous.
- Epidemiology (the way a disease spreads through the population) is not complicated science. The government could have had lots of people who were very good at this but they didn’t.
- We should have cocooned the vulnerable, make sure the NHS has capacity and “let it rip” through the population.
- We should never have had an open-ended lockdown.
- The ‘R number’ is just the difference of in the number of people infected after each generation of a disease. Britain crossed the ‘magical R of 1’ line a few days before lockdown and the same day as Sweden. Whatever interventions have been done doesn’t seem to have had any effect. [See chart 3]
- COVID-19 is mostly a care home and hospital disease. This was obvious very early on. Old people should not have been moved from hospitals into care homes. It seems as if we knowingly seeded the most vulnerable environment with the disease.
- 37% of our deaths are care home residents but they are only 0.5% of our population. Of them are dementia sufferers.
- Over 20% of the infections were picked up in the hospitals. COVID-19 seems more like MRSA than influenza in that it’s an infection control problem.
- COVID-19 is much more comparable to flu for the rest of the population.
- 1968 flu killed 80,000 people in the UK.
- This last winter was a low flu winter. It’s quite possible that the people who died of COVID-19 are those who didn’t die.
- If you overlay COVID-19 deaths with the 2000 flu season, they look very similar. [See chart 4]
- 95% of deaths have had another serious disease. Most people have almost no chance of dying from COVID-19.
- If you are under 40, you have more chance of being struck by lightning that dying of COVID-19.
- If you are under 60, you have more chance of drowning.
- At any age, you have more chance of dying on the roads than dying of COVID-19.
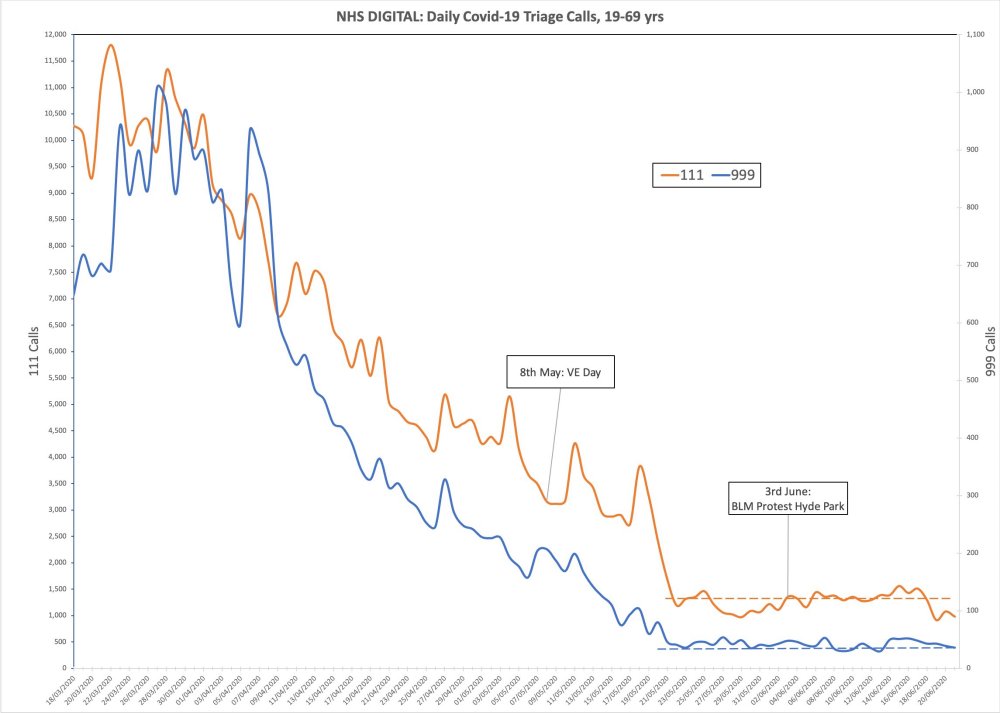
- Lead indicators of 111 and 999 calls with COVID-19 symptoms show there was no spike after VE Day celebrations or BLM protests. In fact, it was even coming down at lockdown. That lockdown was big change for COVID-19 is invisible in the data. [See chart 5]
Charts
Chart 1: COVID-19 was declining in Europe as of march. It was not growing exponentially
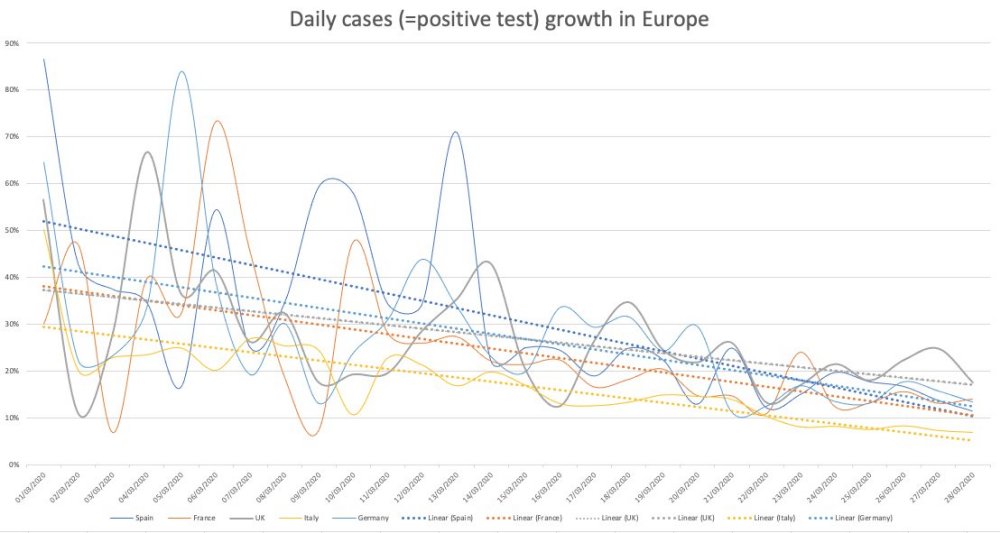
Chart 2: Sweden’s epidemic looks similar to the UK’s but they did not lock down.
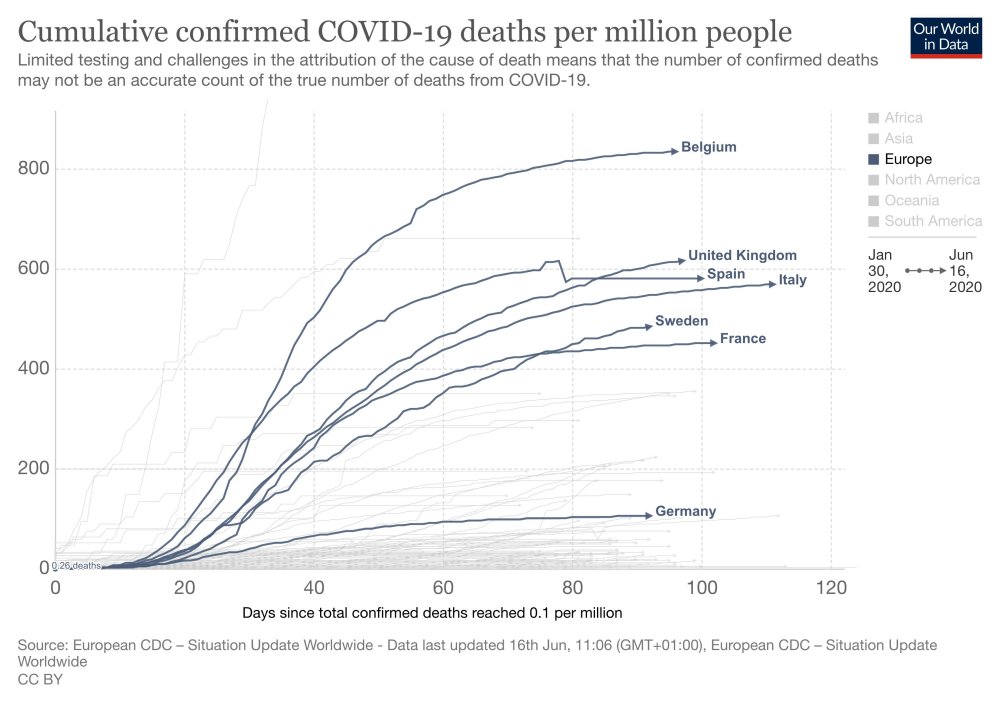
Chart 3: Britain crossed the ‘magical R of 1’ line a few days before lockdown

Chart 4: COVID-19 deaths overlayed with the 2000 flu season
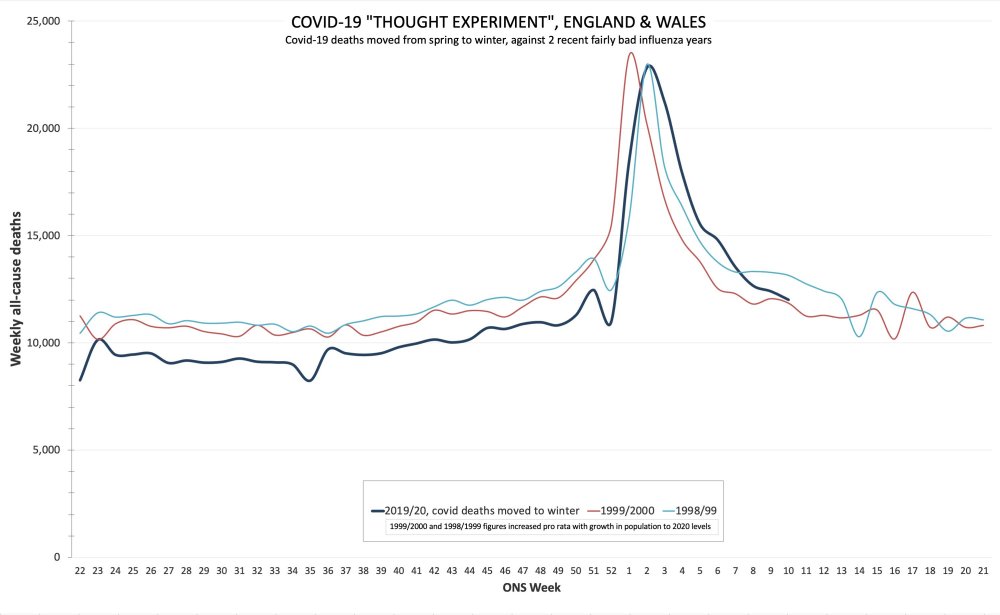
Chart 5: No spike after BLM protests
NHS doctors are prematurely ending the lives of thousands of elderly hospital patients because they are difficult to manage or to free up beds, a senior consultant claimed yesterday.
Professor Patrick Pullicino said doctors had turned the use of a controversial ‘death pathway’ into the equivalent of euthanasia of the elderly.
He claimed there was often a lack of clear evidence for initiating the Liverpool Care Pathway, a method of looking after terminally ill patients that is used in hospitals across the country.
Professor Pullicino claimed that far too often elderly patients who could live longer are placed on the LCP and it had now become an ‘assisted death pathway rather than a care pathway’.
A new report by the National Audit Office confirms that 25,000 people moved from hospitals into care homes between mid-March and mid-April.
Jeremy Hunt, the Conservative former health secretary who now chairs the Commons Health Committee, said the findings were “extraordinary” and came “despite widespread knowledge that the virus could be carried asymptomatically”.
People have died at home alone of Covid-19 during the pandemic and not been found for up to two weeks, doctors who have investigated such deaths have said.
They have only been discovered after a relative, friend or neighbour raised the alarm and have in many cases gone undetected for so long that their body has started to decompose.
It is remarkable how many deaths during this pandemic have occurred in care homes. According to the Office for National Statistics, nearly 50,000 care home deaths were registered in the 11 weeks up to 22 May in England and Wales — 25,000 more than you would expect at this time of the year. Two out of five care homes in England have had a coronavirus outbreak; in the north-east, it’s half.
Not all these deaths, however, have been attributed to Covid-19. Even when death certificates do mention it, it is not always clear that it is the disease that was the ultimate cause of death. The data refers to people who died with Covid-19 present in their bodies, whether or not it was the direct cause. This raises questions about whether there’s another reason for many of these deaths which has gone largely unnoticed while attention has been focused on Covid-19. This is not just a British phenomenon, but one seen across Europe.
https://www.spectator.co.uk/article/dying-of-neglect-the-other-covid-care-home-scandal
Finally, we can say with confidence what many of us have suspected for weeks: not only is the end of the pandemic now in sight but also the people best-placed to recharge our economy have little to fear from it.
Thanks to definitive figures released yesterday by Public Health England, we know that Covid-19 is not a random killer, but one that targets specific groups – namely the old and those with pre-existing conditions such as diabetes or dementia.
Senior social care leaders are calling on ministers to prioritise unlocking care homes amid growing concerns that mental health problems are contributing to the deaths of residents.
In the interest of public debate, we allow visitors to share opinions, experiences and research that may be of value to others. This is a visitor contribution from our Discussions page.
The views expressed are those of the individual posters themselves. Please read our Comments and contributions disclaimer.
Authors
Joyti Valérian Goel
- Website: joytigoel.com
- Contact: [email protected]
Bio: I am of Service to Others, I want to contribute towards the paradigm shift, help people understand what is at stake, to help them make wise decisions, find their paths and progress as human beings.
This document synthesizes practically all aspects of the crisis and that it is to be fully understood once you read it from A to Z because everything is interconnected.
Everybody is entitled to their perspective and has the right to disagree with anything stated in this document. However, I urge you to read the document from A to Z with an open mind before making any decision. I have laid out useful insights and raised pertinent questions in order to appeal to your intellect and instigate enough curiosity so that you can also start researching yourself what is truly going on.
Some of the pertinent question:
• Does the virus exist and if it does, where does it come from?
• Why do so many positive patients suffer from minor or no symptoms?
• What test do they use?
• How do they report a death or a case?
• Why was Italy hit so badly?
• Will things ever go back to normal?
• Are there any links between 5G and the virus?
• What is this pandemic accomplishing?
• Who is benefiting from it?
• What are they hiding from us?
• What can we do?
Download the full paper: https://joytigoel.com/A-Comprehensive-Analysis-of-the-Covid-19-Crisis.pdf
Shockingly, the UK government was not alone in pushing the crisis into care homes. In New York, the centre of the world’s worst outbreak, it is a similar story. Care homes were not only neglected for PPE and testing, but were also ordered to take in Covid patients. Homes could be fined $10,000 or lose their operating licence if they refused to comply with the rules. In Lombardy, the hardest-hit region of Italy, care homes were paid extra to take in Covid patients from hospitals.
The carnage in care homes ought to be the biggest scandal of the Covid crisis.
https://www.spiked-online.com/2020/05/19/how-covid-panic-caused-the-carnage-in-care-homes/
Care home residents confined to their rooms and forbidden visits from loved ones are giving up on life and “fading away”, say staff and families.
“The virus won’t be the killer of these people, it’s the distress and fear of not seeing family that is doing it,” said one carer who asked to remain anonymous but has reported her concerns to the Care Inspectorate in Scotland.
The main thing that went wrong, I believe, was a failure to understand that hospitals would become the vectors for COVID, the epicentres for the infection. We – the hospitals, the decisions taken by the NHS managers with their clipboards – spread the disease, especially among the elderly vulnerable in care homes. A disease that we were trying to stop… killing the elderly and vulnerable.
https://www.rt.com/op-ed/488075-nhs-made-covid-19-crisis-worse/
None of them were healthy at the time they became infected with the virus. “All of the cases had pre-existing conditions and most of them had several,” says Alexandar Tzankov, a pathologist from the University of Basel.
[D]octors found “multiple pre-existing conditions” and they were present “in every single case.” The cause of death tended to be a respiratory tract infection, a lung infection, a pulmonary embolism or a combination of all three. The most common pre-existing conditions found by the pathologists pertained to the cardiovascular system or the lungs.
“Essentially, COVID-19 isn’t a problem to children or the normal, healthy population,” says Püschel. Furthermore, each individual’s physical condition is a more important factor than age, he says. “Age by itself isn’t an illness. Older people are more likely to suffer from illnesses, but the extent of pre-existing conditions is relevant,” Püschel says
The horrible truth is that it now looks like in many of the early cases, the disease was probably caught in hospitals and doctors’ surgeries. That is where the virus kept returning, in the lungs of sick people, and that is where the next person often caught it, including plenty of healthcare workers. Many of these may not have realised they had it, or thought they had a mild cold. They then gave it to yet more elderly patients who were in hospital for other reasons, some of whom were sent back to care homes when the National Health Service made space on the wards for the expected wave of coronavirus patients.
Once the epidemic is under control in hospitals and care homes, the disease might die out anyway, even without lockdown. In sharp contrast to the pattern among the elderly, children do not transmit the virus much if at all. A recent review by paediatricians could not find a single case of a child passing the disease on and said the evidence ‘consistently demonstrates reduced infection and infectivity of children in the transmission chain’. One boy who caught it while skiing failed to give it to 170 contacts, but he also had both flu and a cold, which he donated to two siblings. Children appear to have ACE2 receptors, the cellular lock that the coronavirus picks, in their noses but not their lungs.
https://www.spectator.co.uk/article/we-know-everything-and-nothing-about-covid
It has become clear that a hard lockdown does not protect old and frail people living in care homes—a population the lockdown was designed to protect.3 Neither does it decrease mortality from COVID-19, which is evident when comparing the UK’s experience with that of other European countries.
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31035-7/fulltext#%20
Viruses don’t just go away. This one will never disappear unless and until there is enough exposure to it to produce collective immunity or an effective vaccine appears.
Talk of compulsorily ‘shielding’ (in plain English locking up) the old and vulnerable until one of those things happens is a cruel mockery of basic human values.
About 80% of patients have mild to moderate disease (including non-pneumonia and pneumonia cases), 13.8% have severe disease and 6.1% are critical (respiratory failure, septic shock, and/or multiple organ dysfunction/failure). Individuals at highest risk for severe disease and death are people aged over 60 years of age and those with underlying conditions such as hypertension, diabetes, cardiovascular disease, chronic respiratory disease and cancer. Disease in children appears to be relatively rare and mild. About 2.4% of the total reported cases were individuals under 19 years of age. A very small proportion of those aged under 19 years have developed severe (2.5%) or critical disease (0.2%).
Dr. Wolfgang Wodarg, an epidemiologist and lung disease specialist, explains coronavirus testing.

Update 16 December 2020: This video has been censored from YouTube. An archived mirror is available below.